Merck Serono, the biopharmaceutical division of Merck, announced that The Lancet Oncology has published results from the Phase III trial of its investigational MUC1 antigen specific cancer immunotherapy tecemotide (also known as L-BLP25) in patients with unresectable, locally advanced Stage III non-small cell lung cancer (NSCLC), known as the START trial. Data included in the publication, and first presented at the American Society of Clinical Oncology (ASCO) 2013, showed that the primary endpoint of overall survival (OS) was not met. Median OS was 25.6 months for patients in the tecemotide group compared with 22.3 months for those in the placebo group (adjusted HR: 0. (Xanax) 88, 95% CI 0.75-1.03, p=0.123).
The publication includes an exploratory analysis of a predefined subgroup of patients in the START trial who received tecemotide after concurrent chemoradiotherapy (CRT). Concurrent CRT is a combination of chemotherapy and radiotherapy given at the same time. Patients in this subgroup achieved a median OS of 30.8 months vs. 20.6 months in patients treated with placebo (n=806; HR: 0.78; 95% CI 0.64-0.95; p=0.016). In patients receiving sequential CRT followed by tecemotide or placebo a median OS of 19.4 months was observed for the tecemotide group compared with 24.6 months for the placebo group (n=433; HR 1.12; 95% CI 0.87-1.44; p=0.38).
Tecemotide is an investigational MUC1 antigen-specific cancer immunotherapy designed to stimulate the body’s immune system to identify and target cancer cells expressing the cell-surface glycoprotein MUC1. MUC1 is expressed in many cancers, including NSCLC, and has multiple roles in tumor growth and survival.
Canada needs a national seniors care strategy to respond to issues such as the fast-growing dementia dilemma, according to the Canadian Medical Association (CMA). Dr. Chris Simpson, CMA President-elect, said Canada must move now to invest in a national seniors care strategy and join the 13 countries that already have dementia strategies in place. He added such a strategy is critical to helping our overtaxed health care system cope with about three quarters of a million Canadians already living with Alzheimer’s disease and other forms of dementia. Dementia currently costs the Canadian economy $33 billion a year in direct health-care costs or indirect costs of lost income of family members acting as caregivers. The Alzheimer’s Society of Canada predicts that by 2031, 1.4 million Canadians will have dementia, and by 2040 the annual cost to the economy will reach $293 billion. “We have the dubious distinction of being the only G8 country without a national dementia strategy. Meanwhile, our acute care hospitals are overflowing with patients awaiting long term care placement and our long-term care facilities are understaffed, under-spaced and underequipped to care for our most vulnerable seniors. This leaves patients and their families in limbo, struggling to fill these gaps in our system,” Dr. Simpson said.
Douglas researchers identify first gene involved in adolescent brain development that may play a role in mental health vulnerability. It is known that during this teenaged phase of brain development, adolescents are particularly vulnerable to psychiatric disorders, including schizophrenia, depression and drug addiction. Researchers at the Douglas Institute Research Centre, affiliated with McGill University, have isolated a gene, DCC, which is responsible for dopamine connectivity in the medial prefrontal cortex during adolescence. Working with mice models, they have shown that dysfunction of this gene during adolescence has behavioral consequences which carry into adulthood. The breakthrough provides the first clues towards a fuller understanding of this important phase of brain development. Even subtle variations in DCC during adolescence produce significant alterations in prefrontal cortex function later on. To determine whether the findings of such basic research can translate to human subjects, researchers examined DCC expression in postmortem brains of people who had committed suicide. Remarkably, these brains showed higher levels of DCC expression – some 48 per cent higher when compared to control subjects
A Review Of BHRT Use In Clinical Practice With Respect To Menopausal Concerns
Abstract
This article provides an overview of the scientific literature regarding the safety and efficacy of bioidentical hormone replacement therapy (BHRT) for the treatment of symptoms associated with menopause, including vasomotor symptoms, urinary tract infections, and vaginal atrophy. This review specifically compares safety of bioidentical estrogens and progesterone to conventional hormone replacement therapy (HRT). Data from large randomized controlled trials such as the Women’s Health Initiative (WHI) and the Heart and Estrogen/progestin Replacement Study (HERS) demonstrate detrimental effects resulting from use of estrogen in combination with synthetic progestins. In contrast, data from the large E3N cohort suggest that bioidentical progesterone may offset this risk. Progesterone differs from synthetic progestins in its biological effects on breast tissue, metabolic parameters, as well as on the cardiovascular system. In addition, different routes of BHRT delivery will be discussed, comparing topical and transdermal application methods with oral administration.
Introduction
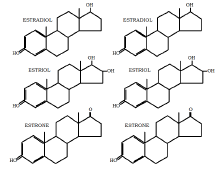
Bioidentical hormones are manufactured to be molecularly identical to endogenous human hormones. They are derived primarily from plant sources, such as soy and wild Mexican yam root. The extracted plant compounds then undergo synthetic processing to obtain structures identical to endogenous human hormones (Bosarge 2009). Some examples include estriol, estradiol, estrone, progesterone and testosterone. There are many commercially available, FDA-approved bioidentical hormones in various forms and dosages. The following products are available: in pill form, Estrace or Innofem; vaginal cream for vaginal symptoms such as Estrace; patches such as Alora, Climara, Estraderm; topical gels Estrogel/Elestrin; and ring forms Estring and Fermin. Progesterone forms include in pill form Prometrium, and as vaginal gel Crinone 4%. Combined formulations include: Combipatch (Estradiol and norethindrone acetate), Prefest (pill) and Limara Pro (patch).
By contrast, synthetic hormones differ structurally compared to human hormones. These compounds typically contain a chemically conjugated functional group to prevent the breakdown of the hormone before it reaches the circulation (Bosarge 2009). Examples include conjugated equine estrogen (CEE) or Premarin, and medroxyprogesterone acetate (MPA).
The following diagrams show the molecular structure of biological estrogens and progesterone, compared to the synthetic forms that are used in conventional HRT and are sometimes referred to as “natural hormones”. The bioidentical hormones have a molecular structure identical to the biological hormones.
Rationale for HRT
The use of hormones in the treatment of peri- and postmenopausal symptoms has a long history dating from the 1960s. Hormone replacement therapy (HRT) is often prescribed to treat symptoms associated with menopause, including hot flashes, sleep disturbance and night sweats (Schmidt 2006). However, since the publication of the Women’s Health Initiative Study (WHI) reporting an increased risk of various cardiovascular events and cancers, many women suffering from peri- and post- menopausal symptoms have turned to the use of BHRT. BHRT is perceived as an effective and safer alternative to conventional treatment with synthetic hormones.
Figure 1. Structure of biological hormones (Left column) compared to synthetics used in conventional hormone replacement therapy (Right column)
Before menopause, ovarian follicles are the source of greater than 90% of estrogen, particularly estradiol. During pregnancy, estriol is the most active form of estrogen. After menopause, the conversion of androstendione to estrone by non-ovarian tissues is the main source of estrogen. Relief of hot flashes in postmenopausal women can usually be achieved by maintaining serum estradiol levels at 40-50 pg/ml, the lowest level of estradiol that is expected to be seen in a typical menstrual cycle (Schmidt 2006). Co-administration of a progestogen is still the standard method used in order to prevent estrogen-induced endometrial hyperplasia (Emons 2004), but co-administration of a synthetic progestin has its own side effects.
Estrogen receptor subtypes
The conflicting results regarding the safety of estrogen use may be in part due to the different forms of estrogen. Each form exhibits different binding affinity and selectivity to estrogen receptors, which is responsible for mediating a different physiologic effect. Estrogenic effects are mediated through two different estrogen receptor subtypes: estrogen receptor-alpha (ER-a) and estrogen receptor-beta (ER- ). ER-a promotes breast cell proliferation, while ER- inhibits proliferation and prevents breast cancer development via G2 cells cycle arrest (Holtorf 2009).
Estradiol equally activates ER-a and ER- , while estrone selectively activates ER-a at a ratio of 5:1. In contrast, estriol selectively binds ER- at a ratio of 3:1(Holtorf 2009). This suggests that estriol is strongly implicated in breast cancer prevention, while the other forms of estrogens may play a role in breast cancer promotion (Holtorf 2009). Due to minimal (<0.4%) conversion of intravenously administered estradiol or estrone to estriol, given its protective qualities, estriol is physiologically important in postmenopausal women. Therefore it is advisable to co-administer estriol with estradiol (Schmidt 2006).
The synthetic counterpart of endogenous estrogens, CEE (Premarin), also selectively binds ER- . Its components are potent downregulators of the ER- receptor subtype that has anticancer effects. In addition, the concomitant use of synthetic progestins along with CEE synergistically down-regulates ER- receptors (Isaksson 2002), which is another possible mechanism underlying the breast cancer-promoting effect of CEE. CEE also contains at least one particularly potent carcinogenic estrogen, 4-
hydroxy-equilenin, which promotes cancer by inducing DNA damage (Holtrof 2009).
In breast cancer survivors, estrogen therapy is especially controversial. However, breast cancer survivors have a high prevalence of severe menopause symptoms due to the induction of a premature menopause with chemotherapy and/or tamoxifen. It is important to find a therapy that is effective and safe for this patient population (Al-Baghdadi 2009).
Progesterone versus progestins
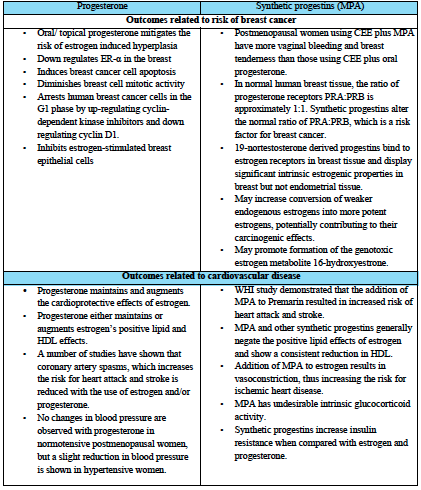
A review of the studies by Holtorf, Opatrny, and L’Hermite reveals that the use of synthetic progestins is associated with a higher risk of cancer compared to bioidentical progesterone (Holtorf 2009, L’Hermite 2008, Opatrny 2008). In particular, two large randomized controlled trials including the Women’s Health Initiative (WHI) and the Heart and Estrogen/progestin Replacement Study (HERS) have shown that use of CEE accompanied by progestins is associated with increased risk of breast cancer (Chlebowski 2003, Hulley 2002). In the WHI study, risk was increased 24% (HR 1.24, 95% CI 1.01–1.54) compared with placebo after 5.6 years (Chlebowski 2003), while in the HERS study, there was a non-significant 27% increase in risk (HR 1.27, 95% CI 0.84–1.94) compared to non-use after six years (Hulley 2002).
Conversely, important data on the protective effects of bioidentical progesterone comes from the French E3N cohort (Fournier 2005, 2008). In this study, Fournier et al prospectively assessed the risk of breast cancer associated with HRT use in a cohort of over 80,000 postmenopausal women (2005, 2008). Compared to non-use, use of estrogen alone resulted in significantly increased risk of breast cancer, HR 1.29 (95% CI 1.02-1.65) (Fournier 2008). However, in combination regimens, this was modified according to the type of progestagen used. As in the RCTs cited above, breast cancer risk was significantly increased by the use of HRT containing synthetic progestins, however in this study there was no increase with HRT containing micronized progesterone (estrogen-progesterone combination) (Fournier 2008, 2005). For example, when analyzing the risk of breast cancer associated with use of transdermal estrogen, estrogen alone was associated with non-significantly increased breast cancer risk, HR1.28 (0.98–1.69); on the other hand, use of transdermal estrogen in combination with the progestins chlormadinone acetate or medrogestone resulted in significant elevations in beast cancer risk, HR 1.48 (1.05–2.09) and 2.03 (1.39–2.97), respectively. Use of transdermal estrogen in combination with bioidentical progesterone however resulted in minimally changed risk compared to HRT non-use, 1.08 (0.89–1.31). An earlier analysis of this cohort, published in 2005, reported a similar relationship. These 2005 findings are depicted in Figure 2. In conclusion, this study suggests that after a mean 8.1 years follow-up, use of bioidentical progesterone conferred protective effects against breast cancer, compared to HRT utilizing synthetic progestins (Fournier 2008).
In a review by Campagnoli et al, further data is reported to the effect that synthetic androgenic (testosterone-derived) progestins might, when combined to estrogens, increase breast cancer risk through androgen-like effects, for instance by increasing IGF-1 activity (2005). IGF-1 exerts potent mitogenic and anti-apoptotic effects on breast cancer cells, in synergy with estrogens. By comparison, use of continuous bioidentical progesterone (100 mg/day), together with transdermal estradiol, failed to increase IGF-1 concentrations over a six month period (Campagnoli 2005). Table 1 summarizes additional evidence comparing the effects of bioidentical progesterone vs. synthetic progestins, as presented by Holtorf 2009 and Schmidt 2006.
Routes of administration
A few studies have investigated the impact of using transmucosal vaginal estrogen preparations on breast cancer recurrence and mortality. The results of these studies are encouraging, demonstrating that topical estrogen usage was not associated with an increased risk of cancer recurrence; however, the need for randomized, controlled trials was emphasized. The lack of convincing evidence that topical estrogen replacement therapy (ERT) increases recurrence and breast cancer-related mortality may encourage clinicians and patients to consider the less potent
According to a review by Holtorf, transdermal estradiol, when given with or without oral progesterone, does not have detrimental effects on coagulation or risk for venous thromboembolism (VTE) (2009). In contrast, there is an increased risk for VTE with the use of CEE (both oral and topical with or without synthetic progestin) (Holtorf 2009). According to the ESTHER study, the relative risk of VTE with oral estradiol was significantly higher than transdermal estradiol. Also, estradiol combined with Norpregnane had a significant increased VTE risk compared with estradiol and Pregnane combination. The lowest observed VTE risk was observed in estradiol with micronized progesterone (L’Hermite 2008).
Minimizing side effects: oral versus topical applications
When using HRT, a generally accepted principle is to prescribe the lowest effective dose on an individualized basis. Topical and transdermal formulations permit application without first-pass metabolism, and may reduce the stimulation of liver production of clotting proteins (Schmidt 2006). For instance, markers of blood clotting risk such as activated protein C resistance that are associated with oral estrogen use are not seen with transdermal administration (Oger 2003). Furthermore, while bioidentical hormones can be administered orally, they have poor oral bioavailability. Rapid metabolism by the liver and the hydrophobic nature of sex steroid hormones suggests that topical administration can be used as an alternative (Minkin 2004). According to Schmidt, transdermal administration of estradiol can maintain serum levels within a relatively narrow range for an extended period of time, with relatively low variation in bioavailability between individuals (2006). For progesterone, the large first-pass effect prevents most orally administered progesterone from reaching the blood plasma and generates metabolites with undesirable side effects; and vaginal bioavailability of progesterone is superior to oral (Schmidt 2006).
Table1. Differential effects of bioidentical progesterone vs. synthetic progestins, based on data reviewed by Holtorf 2009 and Schmidt 2006
A 1998 systematic review of 77 studies evaluating estrogen therapy found that while all routes were effective in the treatment of urogenital atrophy, the form with the least systemic absorption was estriol (administered orally or vaginally), followed by vaginal estradiol, as measured by pre- and post- therapy serum estradiol and estrone concentrations (Cardozo 1998). Side effects of local use are typically limited mild burning or pruritus, which generally disappear after several days of treatment (Raz 2001). Intravaginal estriol is well absorbed. Peak plasma levels of unconjugated estriol after insertion of 0.5mg of cream is comparable with those obtained after 8-12mg administered orally.
Estriol replacement is an effective treatment in the treatment of urogenital complaints related to menopause, and may also have a role in the prevention of recurrent UTIs (Cardozo 1998, Raz 2001). Estrogen reduced vaginal pH and stimulates the proliferation of lactobacillus bacteria which compete with Enterobacteriaceae for vaginal colonization, which are the main pathogens of the urinary tract (Raz 2011). The absence of estrogen decreases the volume of vaginal muscles, resulting in slackness of the ligaments holding the uterus, the pelvic floor, and the bladder, resulting in the development of prolapse of the internal genitalia and predisposing to UTI (Raz 2001). The recommended dose is 0.5mg estriol twice weekly after a loading dose, applied for 14 days to vaginal area.
Compounding BHRT
Bioidentical hormones are commercially available in oral or topical preparations. Examples of commercially available estrogens include Estrace® and Climera®. Compounding pharmacists are able to prepare medications from scratch using individual ingredients that are mixed together to formulate a specific strength of medication (Fugh-Berman, 2007). Compounding bioidentical hormones can provide several advantages such as formulating a preparation to meet the specific needs of the patient. Additionally, BHRT’s can be compounded in various forms such as creams, lotions,PLO gels, capsules, suppositories, troches or patches. Precise dosing allows for individualized treatment based on a patient’s symptoms and responses, avoiding unnecessary side effects (Bosarge 2009). For example, BHRTs can be compounded as a cream containing both estriol and estradiol at a minimum effective dose to minimize unwanted side effects. Convenient dosing and reduction of side effects may improve compliance when compared to conventional hormone replacement therapy (Bosarge 2009). Due to the variability of compounding practices between pharmacies, healthcare practitioners and patients should be cautious when choosing where they fill their medication. Compounding pharmacists can take training courses and receive certifications in compounding practice. It is advisable that physicians refer their patient’s to a reputable compounding pharmacy.
Conclusion
The concept of HRT was initiated in the mid-1960s with the goal of alleviating the symptoms of severe menopause and of cushioning against health risks associated with menopause. However, unease over its use surfaced following findings reported by the Women’s Health Initiative (WHI). Bioidentical hormones offer important benefits over conventional hormone replacement therapy. These include a reduced risk of breast cancer with use of progesterone compared with conventional progestin containing regimens, and lack of detrimental cardiovascular effects associated with progestins. Patients often are confused about the optimal approach to hormone replacement therapy. The choice of compounded bio-identical hormones may be appropriate when FDA-approved products do not provide the option of obtaining the desired medication such as transdermal testosterone; or the desired dose, for instance natural progesterone in a dose <100 mg); or when an allergy precludes an FDA-approved product, such as peanut allergy and Prometrium. Informed MDs, NDs, and pharmacists can help their patient make better decisions based on needs, concerns, preferences, and the best available scientific evidence.
Acknowledgements
The authors wish to thank Joyce Wan B.Sc.Phm and Amin Jagani, BPharm, RPh, MBA for their help and contribution to this paper.
References
Al-Baghdadi O., Ewies A.A.A. Topical estrogen therapy in the management of postmenopausal vaginal atrophy: an up-to-date overview. Climacteric 2009;(12):91-105.4.
Bosarge PM, Freeman S. Bioidentical hormones,
compounding, and evidence-based medicine: what women’s health practitioners need to know. Journal for Nurse Practitioners 2009;5:421-7.
Campagnoli C, Clavel-chapelon F, Kaaks R, Peris C, Berrino F. Progestins and progesterone in hormone replacement therapy and the risk of breast cancer. J Steroid Biochem Mol Biol 2005;96:95-108.
Cardozo L, Bachmann G, McClish D, Fonda D, Birgerson L. Meta-analysis of estrogen therapy in the management of urogenital atrophy in postmenopausal women: second report of the Hormones and Urogenital Therapy Committee. Obstet Gynecol. 1998 Oct;92(4 Pt 2):722-7.
Chlebowski RT, Hendrix SL, Langer RD, Stefanick ML, Gass M, Lane D, Rodabough RJ, Gilligan MA, Cyr MG, Thomson CA, Khandekar J, Petrovitch H, McTiernan A, WHI Investigators. Influence of estrogen plus progestin on breast cancer and mammography in healthy postmenopausal women: the Women’s Health Initiative Randomized Trial. JAMA. 2003; 289(24):3243-53.
Emons G, Huschmand-Nia A, Krauss T, Hinney B. Hormone replacement therapy and endometrial cancer. Onkologie 2004;27:207-210. Fournier A, Berrino F, Clavel-Chapelon F. Unequal risks for breast cancer associated with different hormone replacement therapies; results from the E3N cohort study. Breast Cancer Res Treat 2008;107:103-11.
Fournier A, Berrino F, RiboliE, Avenel V, Clavel- Chapon F. Unequal risks for breast cancer associated with different hormone replacement therapies: results from the E3N cohort study. Breast Cancer Res. Treat. 2008; 107(1):103-111.
Fournier A, Berrino F, Riboli E, Avenel V, Clavel- Chapelon F. Breast cancer risk in relation to different types of hormone replacement therapy in the E3NEPIC cohort. Int J Cancer. 2005 Apr 10;114(3):448-54.
Fugh-Berman A, Bythrow J. Bioidentical hormones for menopausal hormone therapy: variation on a theme. Journal of General Internal Medicine. 2007; 22:1030-1034.
Holtorf K. The bioidentical hormone debate: are bioidentical hormones (estradiol, estriol, and progesterone) safer or more efficacious than commonly used synthetic versions in hormone replacement therapy? Postgrad Med. 2009 Jan;121(1):73-85.
Hulley S, Furberg C, Barrett-Connor E, Cauley J, Grady D, Haskell W, Knopp R, Lowery M, Satterfield S, Schrott H, Vittinghoff E, Hunninghake D, HERS Research Group. Noncardiovascular disease outcomes during 6.8 years of hormone therapy: Heart and Estrogen/progestin Replacement Study follow-up (HERS II). JAMA. 2002; 288(1):58-66.
Isaksson E, Wang H, Sahlin L, et al. Expression of estrogen receptors (alpha, beta) and insulin-like growth factor-1 in breast tissue from surgically postmenopausal cynomolgus macaques after long-term treatment with HRT and tamoxifen. Breast. 2002;11(4):295-300.
Leonetti HB, Landes J, Steinberg D, Anasti JN. Transdermal progesterone cream as an alternative progestin in hormone therapy. Altern Ther Health Med 2005;11:36-38.
L’Hermite Marc, Simonici Tommaso, Fuller Sarah, Genazzani Andrea Riccardo. Could transdermal estradiol + progesterone be a safer postmenopausal HRT? A Review. Maturitas 60(2008)185-201.
Minkin MJ. Considerations in the choice of oral vs. transdermal hormone therapy: a review. J Reprod Med 2004;49:311-320.
Mueck AO, Seeger H. Breast cancer: are estrogen metabolites carcinogenic? Climacteric 2007; 10 (Supple.2); 62-5.
Oger E, Alhenc-Gelas M, Lacut K, Blouch MT, Roudaut N, Kerlan V, Collet M, Abgrall JF, Aiach M, Scarabin PY, et al. Differential effects of oral and transdermal estrogen/progesterone regimens on sensitivity to activated protein C among postmenopausal women: a randomized trial. Arterioscler Thromb Vasc Biol 2003;23:1671-1676.
Opatrny L, Dell`Aniello S, Assouline S, Suissa S. Hormone replacement therapy use and variations in the risk of breast cancer. BJOG 2008; 115:169-175.
Raz R., Postmenopausal women with recurrent UTI. International Journal of Antimicrobial Agents 17 (2001) 269-271.
Raz R. Urinary tract infection in postmenopausal women. Korean J Urol. 2011 Dec;52(12):801-8.
Schmidt JW, Wollner D, Curcio J, Riedlinger J, Kim L. S. Hormone replacement therapy in menopausal women: Past problems and future possibilities. Menopause. Gynecological Endocrinology.2006;22(10): 546-577.
Over six million Canadians are currently affected by hypertension, a primary risk factor for cardiovascular disease. Elevated blood pressure accounts for approximately 13% of all deaths. The Canadian Hypertension Education Program (CHEP) provides annual recommendations for the assessment and management of hypertension in Canada. This article reviews the 2013 CHEP recommendations with a view to their application by integrative healthcare practitioners. For in-office diagnosis of hypertension, if blood pressure is elevated (SBP ≥140 mmHg and/or DBP ≥90 mmHg), it should be re-measured twice more in the same visit. The first measurement should be discarded and the latter two averaged to determine blood pressure. A focused physical exam and history assessing for target organ damage and cardiovascular risk should be performed; and a second visit should be conducted within a month to re-assess blood pressure. Special considerations exist for patients with diabetes and the very elderly. Target blood pressure in diabetics is SBP ≤130 mmHg and DBP ≤80 mmHg; while in patients ≥ 80 years of age it is SBP ≤150 mmHg. The role of integrative medicine in managing hypertension is discussed.
Introduction
Hypertension continues to be the primary risk factor for cardiovascular disease development, leading to myocardial infarction, congestive heart failure, stroke and kidney disease (Chobanian 2003). Worldwide, elevated blood pressure is also the leading risk factor for all cause mortality, accounting for 13% of all deaths (Robitaille 2012). The Framingham Heart Study data suggests that adults who are normotensive at 55 years of age have a 90% lifetime risk for developing hypertension (Vasan 2002), a statistic that warrants considerable emphasis on preventative cardiovascular efforts. The Canadian prevalence of hypertension is growing yearly, with six million diagnosed in 2008; hypertension is most prevalent in Atlantic Canada. Prevalence increases with age and in the female gender (after the sixth decade of life) (Robitaille 2012).
The Canadian Hypertension Education Program (CHEP), operated and funded by Hypertension Canada, provides yearly updates to its recommendations for hypertension assessment and managementin Canada, a feat unmatched by any other country’s task force for hypertension or cardiovascular disease to date. An evidence-based approach is undertaken on an annual basis via systematic review of relevant clinical literature and recommendations are developed and disseminated by key independent stakeholders without external influence. The 2013 CHEP guidelines incorporate new recommendations for special populations suffering with hypertension as well as a greater emphasis on lifestyle and dietary considerations for management (Hackam 2013). These updates are relevant to integrative and conventional practices alike, and provide a more notably holistic approach to hypertension care. This paper will review current Canadian recommendations for blood pressure assessment and management with special attention to the integrative healthcare practitioner’s role in providing best patient care.
Hypertension diagnosis
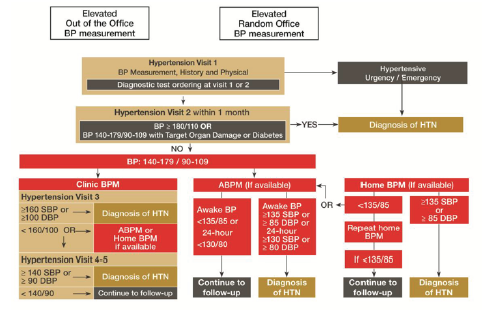
A diagnosis of elevated blood pressure, either in-office or by patient self-report, requires a specific workup based on certain criteria. In order to confirm a diagnosis hypertension, an algorithm for blood pressure measurement has been created
by CHEP 2013, as outlined in Figure 1.
Figure 1. CHEP 2013 Algorithm for the Assessment of Patients with Hypertension (Hackam 2013)
Visit 1: Initial assessment
1. If the initial blood pressure denotes hypertensive urgency or emergency (defined in Table 1), an immediate diagnosis of hypertension is made and treatment is initiated.
2. If blood pressure is elevated (SBP ≥140 mmHg and/or DBP ≥90 mmHg):
a. Re-measure twice more in the same visit. The first measurement is discarded and the latter two averaged to determine visit 1 blood pressure.
b. Schedule follow-up within 1 month for assessment of hypertension.
c. Conduct a focused history and physical examination to assess cardiovascular disease risk and target organ damage (TOD) (defined in Table 2).
d. Assess for contributing exogenous factors and secondary causes of hypertension.
Visit 2: Follow-up assessment
1. If SBP ≥140 mmHg and/or DBP ≥90 mmHg with macrovascular target organ damage (TOD), diabetes mellitus (DM) or chronic kidney disease (CKD), diagnose hypertension.
2. If SBP ≥180 mmHg and/or DBP ≥110 mmHg without macrovascular TOD, DM or CKD, diagnose hypertension.
Visits 3-5: Follow-up assessment
1. If SBP ≥160 mmHg and/or DBP ≥100 mmHg averaged across first 3 visits, diagnose hypertension.
2. If SBP ≥140 mmHg and/or DBP ≥90 mmHg averaged across first 5 visits, diagnose hypertension.
3. If at the last visit the patient does not meet diagnostic criteria, and has no macrovascular TOD, reassess blood pressure yearly.
Table 1. Recognize Hypertensive Urgencies and Emergencies (Hackam 2013)
1. Asymptomatic diastole ≥ 130 mmHg
2. Elevations of blood pressure with:
• Hypertensive encephalopathy
• Acute aortic dissection
• Acute left ventricular failure
• Acute coronary syndrome
• Acute kidney injury
• Intracranial hemorrhage
• Acute ischemic stroke
• Eclampsia of pregnancy
Table 2. Target Organ Damage Examples (Hackam 2013)
1. Cerebrovascular Disease
a. Stroke: ischemia, transient ischemic attack, intracerebral hemorrhage, sub-arachnoid hemorrhage
b. Dementia: vascular, mixed vascular, Alzheimer’s
2. Hypertensive Retinopathy
3. Left Ventricular Dysfunction
4. Coronary Artery Disease
a. Myocardial infarction
b. Angina pectoris
c. Congestive heart failure
5. Renal Disease
a. Chronic kidney disease
b. Albuminuria
6. Peripheral Artery Disease
a. Intermittent claudication
In addition to these general guidelines for hypertension assessment and diagnosis, considerations must be made for certain special populations as defined by CHEP. These groups may not be best addressed by the general recommendations listed above due to physiological and/or clinical differences that affect blood pressure. When patients fall into these groups or subpopulations, it is important to adopt the specific guidelines relating to the implicated subpopulation in order to improve outcomes.
Hypertension and Diabetes
The prevalence of hypertension in diabetic patients is 63%, with 60-80% of diabetics dying from cardiovascular complications largely attributable to hypertension (Campbell 2009). Given the elevated risk of cardiovascular events in diabetics with comorbid hypertension, it is especially important for healthcare practitioners to be aware of their specific blood pressure targets and requirements. Integrative practitioners are specially poised to effectively address this group, given their expertise and ability to provide guidance on dietary and lifestyle modifications that help diminish this risk.
New 2013 recommendations for target blood pressure in diabetics are SBP ≤130 mmHg and DBP ≤80 mmHg (Hackam 2013). This target is based on evidence suggesting that more adverse events and less cardiovascular risk reduction is noted in intensive therapy where SBP targets were ≤120 mmHg vs. standard therapy using SBP targets ≤140 mmHg. Given that diabetics have well-known problems relating to hypo-perfusion, pushing blood pressure too low with treatments may also exacerbate events such as hypotension, syncope, bradycardia, hyperkalemia, angioedema and renal failure, some of which were noted when intensive hypotensive therapy was initiated in this population (ACCORD Study Group 2010).
Hypertension in the Elderly
The new recommendation for isolated systolic hypertension in the very elderly (age 80 years or older) is a target SBP ≤150 mmHg. Arterial thickening is known to occur with increasing age leading to a decrease in vessel elasticity. This physiological process results in systolic elevation with age, a finding that is now being recognized by CHEP guidelines in order to deter overmedication in the elderly population. No changes have been made to the diastolic blood pressure targets, which remain to be recommended ≤90 mmHg (Hackam 2013).
American guidelines note that these patients are more likely to have white coat hypertension and isolated systolic hypertension; in order to address these instances, practitioners should measure seated blood pressure and average two or more readings per visit (Pickering 2005). Additional strategies to circumvent white coat hypertension may include relaxation techniques applied at the discretion of the provider to aid measurement accuracy. Alternate methods for measurement, such as ambulatory and home BP measures, should also be considered.
Laboratory and Diagnostic Tests for Hypertensive Patients
Upon diagnosis of hypertension, the routine investigational laboratory panel should include the following:
*Hypertensive patients with diabetes mellitus should also have urinary albumin assessed (Hackam 2013).
These laboratory measures aid in the investigation of target organ damage from longstanding untreated or inadequately controlled hypertension.
Hypertension treatment considerations
New CHEP guidelines are considerably more holistic in nature compared to previous Canadian guidelines (Daskalopoulou 2012) and currently adopted American guidelines from 2003 (Chobanian 2003). The primary focus of treatment continues to be on healthy behaviour management, including emphasis on physical exercise, weight reduction, alcohol consumption, dietary improvements, and stress management (Hackam 2013).
Pharmacological drug therapy guidelines have also been amended to address the greater shift towards lifestyle modification. The most notable of these changes include the delay of antihypertensive drug initiation for patients who do not have evidence of macrovascular target organ damage or other cardiovascular risk factors. In these otherwise healthy individuals, drug therapy is not recommended until the patient’s blood pressure indicates stage II hypertension, with an average SBP ≥160 mmHg or DBP ≥100 mmHg (Hackam 2013). American guidelines continue to recommend drug therapy initiation for stage 1 hypertensive patients, regardless of cardiovascular risk (Chobanian 2003). In the 2013 CHEP guidelines, stage I hypertension patients are to be recommended lifestyle modification instead.
The debate continues regarding which component of blood pressure is more concerning from the perspective of absolute cardiovascular risk. Recent reviews of evidence point to elevations in systolic pressure and pulse pressure as being most predictive of cardiovascular risk, whereas past epidemiological evidence has typically implicated diastolic elevation as a primary target for antihypertensive treatments (Pickering 2000, Strandberg 2003). Diastolic elevation has historically been regarded as more concerning due to the focus of large clinical trials on diastolic pressure; however more recent studies, including the Framingham Heart Study, confirm that systolic pressure accurately predicts true hypertension 96% of time compared to diastolic readings (Lloyd- Jones 1999). Both Canadian and American hypertension guidelines fail to explicitly distinguish isolated diastolic hypertension from isolated systolic hypertension in their recommendations for assessment, though practitioners should be aware that these do exist. From an evidence perspective, isolated systolic hypertension is a greater concern and requires more aggressive antihypertensive treatments compared to isolated diastolic hypertension. Both of these phenomena are more prevalent in younger patients, often males (Pickering 2000, Pickering 2005).
Lifestyle Recommendations for Hypertension
First line emphasis of treatment for stage 1 hypertension and pre-hypertension includes aerobic exercise and resistance training, neither of which are considered to adversely influence blood pressure. An effort to reduce the contribution of stress to blood pressure and to maintain a normal body weight is also emphasized; an area that integrative practitioners are especially poised to address effectively (Hackam 2013).
Dietary Recommendations for Hypertension
Specific dietary considerations of emphasis for hypertensive patients include sodium restriction <1500 mg for patients under 50 years of age, <1300 mg for those 51-70 years, and <1200 mg for those over 70 years. Alcohol intake should also be moderated in both pre-hypertensive and hypertensive patients, with recommendations for <14 standard weekly drinks in men and <9 standard weekly drinks in women (Hackam 2013). Both of these specific dietary guidelines should be made in conjunction with the recommendation to adhere to the Dietary Approaches to Stop Hypertension (DASH) diet (Appel 2005; Hackam 2013). The DASH diet and Mediterranean diet continue to fare best at reducing absolute cardiovascular risk according to long-term and large-scale clinical trials (Appel 2005, Kokkinos 2005).
Role of Integrative Medicine
The role of an integrative medical practitioner in hypertension assessment and management is variable and diverse. Recent unpublished data reviewing naturopathic management of hypertension in a teaching clinic at the Canadian College of Naturopathic Medicine in North York, Ontario, suggests that a large proportion of practitioners fail to address their patients’ hypertension. The main reason for this trend was patient preference for a focus on other health needs given that their hypertension was being addressed by anti-hypertensive medications and followed by another health professional. Integrative practitioners are often presented with the clinical decision regarding the role played for hypertension management, specifically whether or not to adopt a primary care function in their patient’s hypertension care.
The above considerations are most relevant to a primary care approach to hypertension management, though aspects of these recommendations should be incorporated into any integrative practitioner’s care. Particular emphasis is warranted with respect to special populations of hypertensive patients, such as the elderly, those with diabetes, those with target organ damage and/ or other cardiovascular risk factors, as well as otherwise healthy individuals whose drug therapy may be safely delayed. Many primary and supportive therapies are available for hypertension management whether or not a patient’s blood pressure is medicated or controlled. Knowledge of primary practice guidelines, such as those positioned by CHEP 2013 in Canada (Hackam 2013) and NHBPEP 2003 in America (Chobanian 2003), is crucial to the appropriate care of patients who suffer from hypertension and to the ultimate success of integrative approaches for cardiovascular management.
Take Home Message for the Integrative Practitioner
• Measure blood pressure regularly in adult patients to assess cardiovascular risk
• Use a validated sphygmomanometer, choose an appropriate cuff size, and position the patient for accurate reading
• Understand CHEP recommendations for patients, including special populations with unique blood pressure targets
• Regularly assess for target organ damage.
References
ACCORD Study Group, Cushman W, Evans G, Byington R, Goff D, Grimm R et al. Effects of intensive blood-pressure control in type 2 diabetes mellitus. New England Journal of Medicine. 2010; 362(17): 1575–1585.
Appel L. Dietary Approaches to Prevent and Treat Hypertension: A Scientific Statement From the American Heart Association. Hypertension. 2005; 47(2): 296–308.
Campbell N, Leiter L, Larochelle P, Tobe S, Chockalingam A, Ward R et al. Hypertension in diabetes: a call to action. Canadian Journal of Cardiology. 2009; 25(5): 299–302.
Chobanian A, Bakris G, Black H, Cushman W, Green L, Izzo J et al. Seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension. 2003; 42(6): 1206–1252.
Daskalopoulou S, Khan N, Quinn R, Ruzicka M, McKay D, Hackam D et al. Canadian Journal of Cardiology. 2010; 28(3): 270–287.
Hackam D et al. The 2013 Canadian Hypertension Education Program Recommendations for Blood Pressure Measurement, Diagnosis, Assessment of Risk, Prevention, and Treatment of Hypertension. Canadian Journal of Cardiology. 2013; 29(5): 528–542.
Kokkinos P, Panagiotakos D, Polychronopoulos E. Dietary influences on blood pressure: the effect of the Mediterranean diet on the prevalence of hypertension. Journal of clinical hypertension. 2005; 7(3): 165–70.
Lloyd-Jones D, Evans J, Larson M, O’Donnell C, Levy D. Differential Impact of Systolic and Diastolic Blood Pressure Level on JNC-VI Staging. Hypertension. 1999; 34(3): 381–385.
Pickering T. Effects of Stress and Behavioral Interventions in hypertension – Headache and Hypertension: Something Old, Something New. Journal of clinical hypertension. 2010; 2(5): 345–347.
Pickering T. Recommendations for Blood Pressure Measurement in Humans and Experimental Animals: Part 1: Blood Pressure Measurement in Humans: A Statement for Professionals From the Subcommittee of Professional and Public Education of the American Heart Association Council on High Blood Pressure Research. Circulation. 2005; 111(5): 697–716.
Robitaille C, Dai S, Waters C, Loukine L, Bancej C, Quach S et al. Diagnosed hypertension in Canada: incidence, prevalence and associated mortality. Canadian Medical Association Journal. 2012; 184(1): E49–E56.
Strandberg T, Pitkala K. What is the most important component of blood pressure: systolic, diastolic or pulse pressure? Current opinion in nephrology and hypertension. 2003; 12(3): 293–297.
Vasan R, Beiser A, Seshadri S, Larson M, Kannel W, D’Agostino R, Levy D. Residual lifetime risk for developing hypertension in middle-aged women and men. The Journal of the American Medical Association. 2002; 287(8): 1003–1010.
A complication of long- standing multiple sclerosis (MS)
Abstract
Approximately 85% of patients with multiple sclerosis are first affected by relapsing and remitting disease, with periods of acute exacerbation. The majority of these patients also develop a secondary course of disease, characterized by progressive, gradual loss of function. These two types of disease processes appear to be driven by independent mechanisms, and clinicians should address not only the underlying inflammatory stimuli to reduce periods of exacerbation, but also address targets of chronic neurodegeneration. This article focuses on four key areas with regard to neurodegeneration: mitochondrial dysfunction, cerebrovascular function, iron deposition, and excitotoxicity, to prevent the onset of or decrease the severity of progressive MS.
Over the past five years (2020–2025), one of the most significant advances has been the clinical validation of Bruton’s tyrosine kinase (BTK) inhibitors, which offer promising potential to slow neurodegenerative progression in progressive MS. Notably, tolebrutinib has demonstrated a 31% delay in disease progression in non-relapsing secondary-progressive MS during Phase III trials. Concurrently, fenebrutinib has shown strong suppression of MS activity and disability progression, including early evidence of brain penetration and microglial modulation, with durable effects observed in relapsing and primary progressive MS cohorts. Additionally, emerging research has revealed that neurons within MS lesions accumulate DNA mutations at over twice the rate of healthy neurons, implicating inflammation-driven genetic instability as a contributor to neurodegeneration and opening new therapeutic avenues. These discoveries represent a shift from solely managing inflammatory relapses to also addressing the core drivers of neurodegeneration in long-standing MS.
Introduction
It is well accepted that multiple sclerosis (MS) is a Th1/Th17-mediated autoimmune disease (Korn 2008). In MS about 85% of patients initially experience a relapsing-remitting course of disease (relapsing-remitting multiple sclerosis, RRMS), which is characterized by acute episodes of neurological deficit called “relapses.” These episodes commonly include limb weakness, vision changes, ataxia and sensory disturbances. Relapses are followed by periods of remission, which usually have partial or near-complete restoration of function.
After a variable number of years, the majority of these patients develop a secondary progressive disease course where disability slowly accrues despite often having fewer attacks, suggesting that other mechanisms are involved in progression. Furthermore, commonly used anti-inflammatory medications such as interferon beta have minimal effect on inhibiting the neurological decline, implying that this process is more complex than inflammation alone (Su 2009). Latency to the commencement of progressive MS varies greatly. One study demonstrated a broad range from one to 36 years with a mean of five years in the quickest 25% to greater than 15 years in the slowest 25% (Scalfari 2013). Male sex, older age of onset (>30), and high early yearly relapse frequency (>3) were predictors for more rapid entry into progressive MS (Scalfari 2013). Therefore, because some patients may convert quickly into progressive MS, preventing progressive MS should be a primary goal when treating all MS patients, especially if they are at higher risk.
Relapses are considered to be the clinical manifestation of acute inflammatory demyelination in the CNS, and progression of disability is thought to reflect chronic demyelination, axonal loss and neuronal death (Luessi 2012). MS should be viewed as both an inflammatory and a neurodegenerative condition, which has major implications for therapy; in particular, there is a need for ongoing CNS protection in addition to controlling acute inflammatory exacerbations.
Treatment of Progressive MS
In an attempt to reduce relapse frequency and severity in RRMS patients, I typically employ renditions of the strategies suggested in Table 1. However, it is essential to include neuroprotective strategies in addition to a solid anti-inflammatory, relapse-oriented protocol to delay disease conversion to progressive MS. The following discusses a primarily theoretical approach to reducing the onset and severity of progressive MS by looking at some of the most prominent underlying mechanisms. Unfortunately, many of these have not been studied in humans with the specific endpoint of slowing disability progression. However, I have chosen to present the options that, in my opinion, are theoretically sound for clinical use. I will focus on four key areas that I emphasize in my practice with regard to neurodegeneration: mitochondrial dysfunction, cerebrovascular function, iron deposition, and excitotoxicity, in order to prevent the onset of or decrease the severity of progressive MS.
Mitochondrial Dysfunction
Mitochondrial dysfunction in MS may be mediated by the pathological opening of the mitochondrial permeability transition pore (PTP) located in the inner mitochondrial membrane. The PTP is a channel that activates and opens in response to mitochondrial stress (Su 2013).
In MS, loss of myelin greatly impairs the efficiency of action potential propagation, resulting in mitochondrial dysfunction and damage. The chain of events proceeds: first, in response to demyelination, sodium channels become redistributed along the axon, and their synthesis is upregulated. This results in increased energy requirements to maintain neuronal function. When the demand for ATP exceeds the production capabilities of existing mitochondria, the Na+/K+ ATPases begin to fail. An excess of Na+ ions accumulates within the intracellular space, and eventually this reverses the Na+/ Ca2+ exchanger that normally moves Na+ into the cell and Ca2+ from the cell. Instead, calcium accumulates within the cell. The PTP pore then opens in response to elevated calcium; however, persistent PTP opening leads to loss of the mitochondrial membrane potential, equilibration of ionic gradients, and promotes mitochondrial matrix swelling and outer membrane rupture (Su 2009).
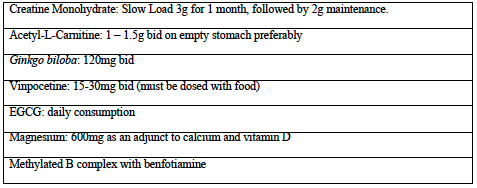
Table 1: Anti-inflammatory strategies targeting relapse severity and frequency
Treatments that increase ATP production may prevent PTP dysfunction. We can attempt to increase ATP production with the use of creatine monohydrate. It is well known that exogenous creatine supplementation provides additional phosphocreatine, which acts as a reserve of high-energy phosphates for ATP production (Rosenfeld 2008). Creatine is taken up by the neuron via specific creatine transporters and phosphorylated to the high-energy phosphocreatine by either mitochondrial or cytosolic creatine kinases (Adhihetty 2008).
Supplying exogenous creatine monohydrate can provide additional substrate for ATP production to meet the increased demand that occurs with demyelination. The activity of creatine monohydrate as a nootropic agent has been demonstrated in healthy adults by supplementing with 5g per day for six weeks, resulting in improvements in working memory (backward digit span) and intelligence (Rae 2003). Creatine has also been shown to maintain the mitochondrial creatine kinase in an octameric conformation. Mitochondrial creatine kinase can exist as either a dimer or an octamer, and the enzyme’s function is determined by its structure (Adhihetty 2008). The octameric form of the mitochondrial creatine kinase interacts with components of the PTP to suppress pore opening and potentially reduce mitochondrial apoptotic susceptibility (Adhihetty 2008). On the other hand, upon exposure to oxidative stress, the enzyme undergoes a conformational change to the dimeric form, losing this functionality (Adhihetty 2008). A “slow load” of creatine supplementation for 28 days at a rate of 3g/day may be considered equivalent to a six-day “fast load” protocol of 20g per day used in athletes, both with a 2g per day maintenance dose thereafter. Based on this, I typically recommend one-half teaspoon for month one, with maintenance of approximately one-third of a teaspoon. Creatine supplementation is easy and convenient as it rapidly dissolves in water and is extremely cost-effective for long-term use.
Acetyl-L-carnitine (ALCAR) is another promising substance that enhances mitochondrial function by facilitating fatty acid transport. To enter the mitochondria, fatty acids must bind to coenzyme A, forming fatty acyl-CoA. Long-chain fatty acyl- CoA molecules are too large to cross the internal mitochondrial membrane and rely on enzymatic transportation that requires L-carnitine (NMCD Carnitine monograph). ALCAR administration results in increased intracellular levels of L-Carnitine. Both IV and oral administration of acetyl-L-carnitine result in a corresponding increase in cerebrospinal fluid concentrations of ALCAR, indicating it readily crosses the blood-brain barrier and can facilitate delivery of additional substrate for ATP synthesis to mitochondria (Alt Med Rev 2010).
ALCAR has been studied clinically in MS patients. Evidence of improved fatigue (implying improved neuronal function) was seen in 36 MS patients who were treated for three months with either amantadine (pharmaceutical for MS fatigue) or ALCAR (1g twice daily); after a three month washout period, the patients were crossed over to the opposite treatment. The authors found that 29% of patients improved after ALCAR compared to 21% after amantadine (Tomassini 2004).
With regards to acute inflammation, ALCAR may also decrease reactive nitric oxide (NO) derivative species. Reactive nitric oxide derivatives are cytotoxic to oligodendrocytes and neurons in culture by inhibiting the mitochondrial respiratory chain. MS patients are known to have increased nitrosative stress, as activated glia secrete reactive nitrogen species (Bizzozero 2005). In a clinical trial, ten MS patients were treated for six months with 2g ALCAR and compared to untreated MS subjects or patients with non-inflammatory neurological conditions. Prior to treatment, concentrations of reduced glutathione were approximately 38% lower in MS patients compared to controls, implying increased baseline inflammatory activity. Treatment with ALCAR resulted in decreased CSF levels of NO reactive metabolites as well as increased content of reduced glutathione (Calabrese 2003).
In my experience, the effects of ALCAR on MS fatigue are subtle, however, it is an extremely well tolerated intervention, and provides acute inflammatory as well as chronic metabolic support. A dose of 1.0- 1.5g bid is a common recommendation.
Dosing on an empty stomach is recommended, to maximize its absorption in the jejunum (Alt Med Rev 2010).
Cerebrovascular Function
CCSVI (cerebrospinal venous insufficiency) is an area that MS patients often inquire about. CCSVI refers to the idea that blocked extracranial venous blood outflow causes cerebral venous reflux in MS patients. It seems now that scientific evidence supporting a causal relationship between CCSVI and MS is lacking. If MS is associated with CCSVI, it is most probably an acquired phenomenon that occurs particularly in MS patients associated with age (Lanzillo 2013). Nonetheless, in my practice I have observed substantial improvements in neurological function in some patients following CCSVI surgery, and from a non-surgical perspective, it is well known that cognition improves among non-MS patients following use of naturally occurring nootropics that improve blood flow, such as ginkgo. Ultimately, whether or not impaired blood flow is an etiological phenomenon in MS, improving cerebral circulation remains an important area of focus when addressing neurodegeneration; improved circulation results in improved oxygen and nutrient delivery to neurons experiencing increased energy demands. The two agents I use often are Ginkgo biloba and Vinpocetine.
In MS patients, ginkgo has been shown to improve both functional and cognitive parameters when dosed at 240mg per day (Johnson 2006, Lovera 2007). The Johnson study used an extract standardized to 24% flavonoid glycosides, 6% terpene lactone (2006), while the Lovera study used an extract standardized to 31.4% flavonoids, 4.5 % terpenes (2007). Neuroprotective effects of ginkgo have been demonstrated in several in vitro and in vivo models, specifically showing protection of cultured neurons against death induced by hypoxia, glutamate and nitric oxide (Ahlemeyer 2003). Ginkgo also appears to have IL-6 lowering ability when given to patients with age-related neurological disorders (Ching-Hsiang 2012). Interestingly, ginkgo appears to be able to increase endothelial nitric oxide synthase (eNOS) mediated NO production, resulting in vasodilation, whereas it inhibits inducible NOS (iNOS) mediated NO production, thereby preventing excessive NO synthesis by macrophages (Ahlemeyer 2003). This suggests that Ginkgo may reduce acute inflammation while providing increased blood flow to damaged neurons. My preference has been to dose Ginkgo at 120mg bid (standardized to 24% and 6%) because it’s readily available at this standardization, and reflects the dose used in Johnson (2006).
Vinpocetine is an interesting substance due to its ability to increase blood flow, as well as its therapeutic potential in neurogenic bladder. In one study, intravenous vinpocetine increased both global and regional cerebral blood flow, with 36% and 37% increases in blood flow to the thalamus and caudate nucleus respectively, as measured by positron emission tomography (PET) (Szilágyi 2005). An oral dosing study using PET imaging also demonstrated increased cerebral blood flow as well as improvements in cognition in patients with mild cognitive impairment due to cerebral hypoperfusion (Valikovics 2007).
Vinpocetine has also been studied for bladder dysfunction. In a pilot study of 19 patients with urge incontinence, sensory incontinence and low compliance bladders, three patients reported slight improvement, and eight reported pronounced improvement within four weeks (Truss 2000). MS patients with neurogenic bladder are considered motor urge incontinent (overactive detrusor). A larger follow up trial in a “worst case scenario population” with primarily detrusor instability showed less pronounced benefits (Truss 2001). Both the vascular and bladder related improvements are attributed to vinpocetine’s phosphodiesterase-1 inhibitory activity. Viagra is a pharmaceutical phosphodiesterase-5 inhibitor (Truss 2001). Phosphodiesterase inhibitors (PDEIs) suppress TNF-alpha production by various cells and suppress experimental demyelination. In a pilot study of 12 MS patients, a combination of three PDEIs was shown to reduce annual relapse rates (Suzumura 2000). Under fasting conditions, vinpocetine has about 7% bioavailability so it must be given with food (Paytar 2011). I typically dose 45mg per day, however 30-60mg is suggested by a 2003 Cochrane review as being suitable for cognitive impairment (Szatmari 2003). Emprical use of vinpocetine for bladder function should be for at least one month, as results were seen within one month in the study by Truss (2000). Precautions related to risk of bleeding relate to both ginkgo and vinpocetine (NMCD Vinpocetine monograph).
Iron Deposition
Zamboni’s CCSVI theory proposed that venous reflux leads to iron deposition, inflammation and leukocyte infiltration. Regardless of whether the CCSVI hypothesis is correct, iron is in fact implicated in a number of neurodegenerative diseases and senile dementia since it accumulates in the brain with age, and ionic iron can in turn participate in the Fenton reaction with subsequent generation of ROS, initiating the processes of oxidative stress (Singh 2009, Weinreb 2009).
In one study, the brain tissue of 33 MS and 30 control cases were analyzed. In active MS lesions, iron was apparently released from dying oligodendrocytes, resulting in extracellular accumulation of iron and it was suggested that cellular degeneration in MS lesions leads to waves of iron liberation, which may further propagate neurodegeneration (Hametner 2013).
In mice being fed oral EGCG, a human equivalent dose of three litres of green tea, dramatically suppressed experimental autoimmune encephalomyelitis (EAE, the animal model of MS) (Atkas 2004). EGCG inhibits Th1 and Th17 differentiation, NF-kb, and ROS, making it one of my top choices for use in reducing relapse severity and frequency (Wu 2012). However, in the context of neurodegeneration, EGCG can also chelate ionic iron to form inactive complexes (Weinreb 2009).
Interestingly, a recent study has shown in-vivo synergy of EGCG and copaxone (daily injectable immune-modulating MS treatment) in EAE, and the authors encouraged the combination of anti-inflammatory and neuroprotective treatments (Herges 2011). Converting the mouse EGCG dose (300 ug bid) used in the first EAE study to an equivalent human dose (assuming 60kg human and 20g mouse) yields approximately 1459mg EGCG as the therapeutic human dose (Mouse-Genome 2010, Reagan-Shaw 2008).
Although there are many factors to be considered in extrapolating animal dosages and their effects to humans, this study does
provide a loose estimate. In practice, I dose EGCG at about 900mg per day when trying to reduce relapse frequency or as an adjuct to interferon, since dosing of EGCG alone at 800mg is a dose that has consistently been shown to be safe in a human pharmacokinetic study. There have been case reports of hepatotoxicity with EGCG, which suggest some caution should be used with higher dosages. The other catechins present in green tea extract possess similar properties to EGCG, and can be used to help make up the full catechin dose used in the EAE study (Chow 2003, Shanafelt 2009). In terms of using EGCG to prevent neurodegeneration, I encourage, at the very least, daily ad libitum consumption of green tea beverage to ensure some degree of iron chelation as part of their neuroprotective regime.
Excitotoxicity
Evidence has accumulated that excessive glutamate is released at the sites of demyelination and axonal degeneration in MS plaques, and the most probable candidates for this cellular release are infiltrating leukocytes and activated microglia (Frigo 2012). One study looking at MS patients compared to healthy patients, found the presence of elevated glutamate in active lesions using 3D MRI. One of the primary glutamate receptors, the NMDA receptor, allows the influx of cations, though most notably calcium. Excessive glutamate stimulation causes excessive intracellular calcium accumulation, leading to excitotoxic injury (Lau 2010). One study looked at 16 patients with MS, where one year without treatment was followed by 1-year riluzole (inhibits glutamate release from neurons). Treatment resulted in reduced spinal atrophy and reduced T1 lesions (active lesions) (Killestein 2005). Although pharmacologic glutamate inhibitors are not currently being employed for this, we can use natural glutamate antagonists to combat the excitotoxicity. GABA receptors provide a counterbalance to glutamate receptors (Rossi 2012). My preference is to use daily magnesium as an adjunct to calcium supplementation; magnesium is a NMDA antagonist and GABA-A agonist, and I have seen good effects in MS spasticity with this approach (Held 2002). I always combine calcium with vitamin D prescription. As mentioned in Table 1, I often recommend 10,000 IU of vitamin D daily in MS. Studies of EAE and a 2010 human dose escalation study where doses reached 40 000 IU indicate that the immune modulatory actions of vitamin D may be contingent on concomitant calcium administration (approximately 1200mg) (Burton 2010, VanAmerongen 2004). As a result, I regularly suggest 10,000 IU vitamin D, 1200mg calcium, and 600mg magnesium nightly. The anxiolytics GABA and taurine can also be considered, especially if anxiety is part of the symptomatology, since taurine is a GABA agonist and may have independent neuroprotective effects, while GABA promotes specific patterns of brain activity (Abdou 2006, Oja 2007).
Table 2: Proposed Strategies for Progressive MS (Neurodegeneration)targeting relapse severity and frequency
Lastly, as a foundation for more advanced supplement therapies, B-vitamins and a diet including daily berry consumption are often prescribed for general cognitive function. A B complex with methylated B12 and benfotiamine is preferred for homocysteine reduction and optimal nerve transmission. Lower median CSF vitamin B12 concentrations were found in groups of patients with MS and serum homocysteine is significantly increased in MS patients (Niist 1990, Vrethem 2003). Blueberry consumption has been shown to improve memory in older adults, has been shown to improve blood brain barrier integrity, and can suppress NF-kb by about 27% in humans when used at a dose of 200g daily (Karlsen 2007, Krikorian 2010, Robert 1977).
Promising prospective therapies that I may add to my formulary in future include: low dose lithium orotate, pyrroloquinoline quinone (PQQ), and Centella asiatica for their effects on brain derived neurotrophic factor (BDNF), nerve growth factor (NGF) and nerve regeneration respectively (Misra 2012, Rowe 2004, Soumyanath 2005). I look forward to more research emerging on the possible role of these agents.
In conclusion, MS should be treated as both an inflammatory and neurodegenerative condition. RRMS patients need neuroprotective support immediately, alongside their immune modulatory therapies, because the onset of progressive disease varies greatly and can even be immediate (primary progressive). It is my opinion that neuroprotective strategies addressing mitochondrial dysfunction, iron deposition, excitotoxicity, and vascular perfusion, in addition to anti-inflammatory treatments, are a well-rounded approach to reducing the possibility and severity of progressive disability accrual.
Great ingredients have always been at the heart of everything Aubrey does. Here’s what else has contributed to their ongoing success over nearly half a decade.
Great ingredients make great products. This is the message at the heart of everything Aubrey does. “Why use a petrochemical ingredient when a natural, plant-base ingredient works so much better?” asks Curt Valva, CEO and president.
Aubrey has thrived for 46 years as a business by providing all-natural, safe and effective personal care products to the consumer. “We offer a true and authentic alternative to many of the mass produced synthetic products on the market today,” says Valva. “We craft the highest quality natural products without compromise as to ingredients, packaging or cost.”
The company believes that we are all citizens of the world and should, therefore, accept the responsibilities that accompany that. “We work with farm communities, suppliers and businesses from around the world,” says Valva. “Whether sponsoring organic agriculture in Honduras, overseeing the development of herbs in Japan, or explaining the importance of organic farming techniques in Ghana, our commitment to people and to the earth is profound.”
Quality and Purity Reign
Aubrey’s commitment to making pure, wholesome, petrochemical-free products runs deep. Since the founder’s passing in 2011, the company has continued to stay true to his mission of clean, all-natural ingredients and purity in manufacturing. Before taking over as CEO and President of Aubrey Organics, Inc., Curt Valva worked closely with Aubrey for more than 12 years, sourcing natural and/or organic ingredients from all over the world.
A well-trained staff of over 50 employees with an impeccable work ethic is also a key component. From research and development in the lab, to the mixing of the products (always by hand, in small batches of 50 gallons or less to guarantee freshness), to the packaging process (using recyclable plastic bottles and boxes made with as much recycled materials as possible), Aubrey’s employees continue to make sure the Aubrey name remains synonymous with quality and purity.
Product Development
Any new formulations are shaped by Aubrey Hampton’s vision, blending centuries’ old herbal traditions and new science. It all begins with extensive study in the lab. Recently Aubrey spent the better part of two years researching new ingredients and developing the products that make up their new skin care line. As a result, the line now features over a dozen tested (on human subjects—Aubrey never tests on animals) and clinically proven new ingredients, in addition to the herbal and plant extracts they’ve been using for years. Following in Aubrey Hampton’s footsteps, the company is committed to utilizing the latest technologies while remaining true to their core philosophy that natural is always best.
To bring these ideas – new and old – to the next generation of retailers, the company will rely on education and transparency. “Part of our core purpose is to provide retailers with as much information about our products as possible,” says Valva. That will happen through printed materials like brochures, sales manuals, and Aubrey’s INCI Dictionary of Natural Ingredients. Social media and the extensive educational section on the company website Aubrey-organics.com will also play a huge role. “We believe if we provide both retailers and consumers with valuable information, they will be able to make an educated purchasing decision,” says Valva. “We believe they will choose Aubrey.”
Aubrey also believes that giving their products a fresh, contemporary look will make them stand out on store shelves. “Our new packaging is designed to reach out to a new generation of retailers and consumers and keep our brand relevant in the marketplace,” says Valva.
How would the Canadian market be approached?
Canada is a very unique market, different from other markets worldwide. “It is a culture based on ethics and morals, where deals can still be made on a handshake,” says Valva. “There are some obvious differences, pertaining to climate and geographic challenges, however, we try to reach each and every customer personally.”
Aubrey has sold their products in Canada for more than 30 years, so they are very familiar with the diversity of the Canadian market. In addition, Valva lived and worked in Canada for many years. “We know Canadian customers are very concerned with quality products and the specific functions of ingredients,” says Valva. “They are smart, educated consumers willing to invest in their personal health and well-being. We try to match our strengths to each customer on a personal basis by offering a premium quality product using only the best certified natural and/or organic ingredients possible.”
Aubrey’s primary reach is coordinated between their distribution partners (Purity Life), the store groups and the Canadian consumer at large. They are planning an extensive advertising campaign, with ads in consumer and retailer publications throughout Canada. They also attend and have a strong presence in Canadian natural product trade shows, with sample giveaways, product demonstrations and show deals.
As mentioned earlier, social media plays an important role in Aubrey’s promotional strategy. The marketing team regularly sends out notifications and updates through Facebook and Twitter to get digital consumers excited about Aubrey products. Aubrey also has a long list of faithful customers who subscribe to their monthly email blasts, which feature updates and special deals on new and existing products.
Lastly, they provide sample packets of many of their new products for stores. This gives customers and retailers risk-free trials of exciting new products, such as their new skin care line.
“Ultimately, we believe the best accomplishment of a successful organization is to make the world a little better, a little cleaner, a little brighter than we found it,” says Valva. Consumers can see the authenticity in Aubrey and that alone helps when they’re making their purchasing decisions.
Genetic engineering researcher has a change of heart – and mind
By Denise Deveau / Photographs by Angela Fama
For Dr. Thierry Vrain, it wasn’t an “aha” moment that ignited his passion for dispelling the genetically engineered (GE) myths. In fact, his journey was decades in the making.
Vrain was a respected researcher and proponent of GE for years. Now retired, he spent more than 20 years in biotechnology research with Agriculture Canada where his focus was on creating parasite-resistant potatoes, raspberries and strawberries, among other foods. However, Vrain’s post-retirement years led him to question the decades of work that he had put into agricultural research, and he’s ready and willing to talk about those doubts.
He admits that the early days of genetic engineering were exciting and dynamic for scientists like him. “Biotech was where the money was. It was easy to get funding, the technology was powerful, and the sky was the limit. You could do miracles working with DNA. I don’t recall ever having reservations about the work we were doing because we were learning to protect crops.”
Throughout his career he had often encountered the argument for organics, but he wanted to see facts supporting the claim. “Because I was a scientist, throughout my career organics seemed like a religious cult. There was no data or evidence anywhere to show it was any better than conventional methods. The only difference was the yields were lower.”
Those numbers presented themselves in 2002, when he came across research papers from Europe on organic methods for growing food. “Seeing documents speaking a scientific language was a turning point for me. Because I’m a cell biologist, what was said in these studies about synthetic fertilizers damaging soil biodiversity made sense to me. There was a noticeable difference,” he says. “So I started becoming more and more interested and I realized that maybe genetic engineering was not all that good. Research from Europe, especially, is clearly showing some very serious problems.”
Part of that can be explained by conclusions that came of the Genome Project, which wrapped up in 2002. All of a sudden, the genome wasn’t at all what scientists thought it was, Vrain says.
The project determined that the human genome has 25,000 genes, but there are 100,000 proteins in the human body. “Everybody expected to see 100,000 genes. Instead, we learned that a gene can make more than one protein – and that’s very important, because proteins are the enzymes that work within cells that make life possible.”
The fact that a single gene sequence will create more than one protein translates into more than one activity. “When we alter that by genetic engineering, we don’t know what unexpected problems we could be creating,” he says. “Many studies now show that the protein you expect to see is either not there or has been truncated, altered or mutated.”
This counters 60 years of research in genetic engineering, Vrain notes. “GE is rooted in a very naïve understanding of genetics because it was based on a one gene/one protein hypothesis that was started when DNA was discovered in the late 1940s. Now we are realizing that introducing genes into a genome could introduce instability, creating proteins that should not be there. Right now we don’t know what they do.”
The specific genetic engineering technology he speaks to is the one that allows plants to be sprayed with herbicide so that the weeds disappear and the plants continue to grow. The problem, however, is that the residue of that herbicide remains on the plant.
The consequences of this are far-reaching, since over 90 per cent of all those plants today are engineered to resist the Roundup herbicide, Vrain says. “When I was a grad student, Roundup was very new. It was non-toxic and biodegradable. We thought it was like water and as safe as aspirin.”
While those properties hold true, it’s the mode of action that has long-term consequences, he argues. By way of explanation, Roundup uses a chelating agent that captures metal ions. The chelation process was originally developed to clean up heavy metals in industrial wastewater, and was eventually used as a broad spectrum herbicide to kill weeds. “A chelating agent competes for metals so enzymes can be impaired, but many proteins need metal ions to function,” Vrain says.
As a result, genetically engineered foods contain residues of antibiotics. “While high or low residues of antibiotics won’t kill you instantly, over time it does damage flora for all animals, because there are 100 billion bacteria in each human’s gut,” he explains.
This is where European studies are showing some intriguing long-term outcomes. “They’re indicating definite organ damage on mice and rats after many months, which would mean many years for a human being,” he says. “There’s no denying that a large number of epidemic chronic diseases are on the rise in the last 20 years. If you put two and two together, there is a probable connection that herbicide residue and engineered crops could be contributing factors to that,” Vrain notes.
For those that argue the need for genetically engineered crops to feed the world, Vrain’s response is, “Industry will say after so many years and many trillions of meals, no one is harmed. But there is no evidence to provide [for] that. It’s empty.”
When not running his “super organic” farm on Vancouver Island, Vrain is increasingly being asked to present his views on genetic engineering, including an appearance on TED Talks. He has decided to join Dr. Shiv Chopra, a former Health Canada scientist who lost his job after going public with concerns about the potential human health risks associated with bovine growth hormone (rBGH), for his first-ever cross country speaking tour running through to February 2014. The “Genetically Engineered (GE) Foods and Human Health: A Cross-Canada Speaker’s Tour” is being held by the Society for a GE Free BC and Greenpeace Vancouver Local Group.
For Vrain, the writing should be on the wall for genetically engineered foods in North America. To date there has been legislation in Europe and other jurisdictions banning their use, yet North America continues to operate in a biotech bubble, he says. “There has never been any testing done in the U.S. or Canada by regulatory agencies, only by corporations, but most of the world has burst that bubble already.”
While Vrain doesn’t have a definitive answer on where the research will take them, “My conclusion would be that the future of agriculture is not genetic engineering.”
Vitality Products Inc. is pleased to announce the revitalization of one of Canada’s oldest natural health companies with the launch of Vitality’s new line of vitamins and supplements. The Company, a manufacturer and marketer of premium quality natural health products, has formulated, branded and launched four products in key growth categories: multivitamins, digestion, stress and sleep. The four unique products announced are Vitality introduces: Vitality® Time Release Super Multi+TM, Vitality® Time Release B Complete + CTM, Vitality® Digest+TM and Vitality® Relax+TM. All four products are non-GMO (contain no genetically modified organisms), gluten-free, soy-free and vegan friendly. Vitality named the four products by their benefits to help retailers and consumers understand the products and added QR codes on labels to direct consumers online for additional product information. Vitality’s new branding, products and product information are available at the Company’s website: www.vitality.ca.
Working Canadians average less than eight hours of sleep each night, are tired and unproductive on the job. A new Canadian survey from Breathe Right®Nasal Strips reveals ninety per cent of adults have experienced a poor night’s sleep, and nearly 40 per cent of survey respondents report they generally do not get a good night’s sleep. Adults ages 35-64, typically in the prime of their careers, are most likely to average less than six hours of sleep per night. The result is a tired, unmotivated, unproductive workforce that is willing to give up evening entertainment, sex, vacations days – and even a raise – just to get a good night’s sleep.