






The current dose-response meta-analysis was conducted to summarize the evidence regarding the association between magnesium intake and stroke risk since prospective studies have yielded inconsistent results. Relevant prospective studies that reported RRs with 95% CIs of stroke for ≥3 categories of magnesium intake were identified by searching PubMed and EMBASE from 1966 through 2011 and by reviewing reference lists of retrieved articles. Results from individual studies were combined using a random-effects model. Seven prospective studies with 6,477 cases of stroke and 241,378 participants were eligible for inclusion. A modest but statistically significant inverse association was observed between magnesium intake and risk of stroke. An intake increment of 100 mg Mg/d was associated with an 8% reduction in risk of total stroke (combined RR 0.92; 95% CI 0.88-0.97), without heterogeneity among studies (P = 0.66; I2 = 0%). In addition, magnesium intake was inversely associated with risk of ischemic stroke (RR 0.91; 95% CI 0.87-0.96) but not intracerebral hemorrhage (RR 0.96; 95% CI 0.84-1.10) or subarachnoid hemorrhage (RR 1.01; 95% CI 0.90-1.14). The authors concluded that dietary magnesium intake is inversely associated with risk of stroke, specifically ischemic stroke. Am J Clin Nutr. 2011 Dec 28. PMID: 22205313
Low red blood cell omega-3 fatty acid levels are associated with accelerated brain aging

This study examined the cross-sectional relation of red blood cell (RBC) fatty acid levels to subclinical imaging and cognitive markers of dementia risk in a middle-aged to elderly community-based cohort (N = 1,575; 854 women). RBC docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA) levels in dementia-free Framingham Study participants were related to performance on cognitive tests and to volumetric brain MRI, with serial adjustments for age, sex, and education, additionally for APOE 4 and plasma homocysteine, and also for physical activity and body mass index, or for traditional vascular risk factors. Participants with RBC DHA levels in the lowest quartile had lower total brain and greater white matter hyperintensity volumes when compared to others (P = 0.009 and P = 0.049, respectively) with persistence of the association with total brain volume in multivariable analyses. Participants in the lowest quartile of DHA and ω-3 index (RBC DHA+EPA) levels also had lower scores on tests of visual memory (P = 0.008), executive function (P = 0.004), and abstract thinking (P = 0.004). Therefore, lower RBC DHA levels are associated with smaller brain volumes and a “vascular” pattern of cognitive impairment in a dementia-free elderly population. Neurology. 2012 Feb 28;78(9):658-64. PMID: 22371413
Two probiotic strains improve immune function in an influenza vaccination model

This randomized, double-blind, placebo-controlled, parallelgroup study investigated the ability of Bifidobacterium animalis ssp. lactis (BB-12®) and Lactobacillus paracasei ssp. paracasei (L. casei 431®) to modulate the immune system. Healthy subjects (n = 211) consumed a minimum of 109 colony-forming units of BB-12® (capsule) or L. casei 431® (dairy drink) or a matching placebo once daily for six weeks. After two weeks, a seasonal influenza vaccination was given. After six weeks, changes in vaccine-specific plasma IgG, IgG1, and IgG3 were significantly greater in both probiotic groups versus placebo (L. casei 431®, P = 0.01 for IgG; P < 0.001 for remaining comparisons). The number of subjects obtaining a substantial increase in specific IgG (≥ 2-fold above baseline) was significantly greater in both probiotic groups versus placebo (BB-12®, P < 0.001 for IgG, IgG1, and IgG3; L. casei 431®, P < 0.001 for IgG1 and IgG3). Significantly greater vaccine-specific secretory IgA levels in saliva were observed in both probiotic groups versus placebo (BB-12®, P = 0.017; L. casei 431®, P = 0.035). Similar results were observed for total antibody concentrations but no differences were found for plasma cytokines or innate immune parameters. Br J Nutr. 2012 Mar;107(6):876-84. PMID: 21899798
Antioxidant supplements for prevention of mortality: systematic review

This systematic review investigated the effects of antioxidant supplements on prevention of mortality in adults. The Cochrane Library, MEDLINE, EMBASE, LILACS, the Science Citation Index Expanded, and Conference Proceedings Citation Index- Science were searched. Seventy-eight primary and secondary prevention randomized clinical trials (N = 296,707) on antioxidant supplements versus placebo or no interventions were included. Overall, antioxidant supplements had no significant effect on mortality in a random-effects model but significantly increased mortality in a fixed-effect model. In 56 trials with a low risk of bias, antioxidant supplements significantly increased mortality (RR 1.04; 95% CI 1.01-1.07). Excluding factorial trials with potential confounding, 38 trials with low risk of bias demonstrated a significant increase in mortality (RR 1.10; 95% CI 1.05-1.15). In trials with low risk of bias, beta-carotene (26 trials; RR 1.05; 95% CI 1.01-1.09) and vitamin E (46 trials; RR 1.03; 95% CI 1.00-1.05) significantly increased mortality, whereas vitamin A (12 trials; RR 1.07; 95% CI 0.97-1.18), vitamin C (29 trials; RR 1.02; 95% CI 0.98-1.07), and selenium (17 trials; RR 0.97; 95% CI 0.91-1.03) did not significantly affect mortality. Dose of vitamin A was associated with increased mortality (P = 0.002). Cochrane Database Syst Rev. 2012 Mar 14;3:CD007176. PMID: 22419320
The overweight/ obesity epidemic revisited

The overweight/ obesity epidemic revisited
Low fat, low carb, or Mediterranean?
Abstract
The prevalence of obesity is of monumental concern and has been growing at an exponential rate over the last few decades. Abdominal adiposity is associated with cytokine perturbations leading to prothrombotic and proinflammatory states and these metabolic changes promote cardiometabolic complications. To date, body mass index (BMI) has been strongly and positively linked to an increase risk of type 2 diabetes, cardiovascular disease, sleep apnea, osteoarthritis, dyslipidemia, asthma and certain cancers. Aside from increased co-morbidities obese and overweight populations have a decreased life expectancy compared to their normal weight counterparts. Modest caloric restriction based on energy expenditure is favored long-term over very low calorie diets. Dietary interventions based on macronutrient proportions alone seem over simplistic and fail to demonstrate any clinically relevant difference in weight loss. Weight loss in general improves cardiometabolic parameters; however, no other diet supports the primary and secondary improvement of hard outcomes such as cardiovascular mortality and all-cause mortality as the MedDiet. Both the Mediterranean Diet (MedDiet) and a Low Glycemic Diet (LGD) show effective weight loss results as well as important improvements in common comorbidities. A modified low-glycemic MedDiet includes smaller more frequent meals, moderate consumption of healthy fat (olive oil), high intake of vegetables and fruit, low quantities of red meat using poultry and fish to replace beef and lamb, and the inclusion of high fiber, LG whole grains. Obesity must be viewed as a chronic condition since weight regain is common. A maintenance dietary program, continual support and behavioural strategies are critical for long-term success.
The prevalence of obesity is of monumental concern and has been growing at an exponential rate over the last few decades (WHO 2002). In 2004, according to the Canadian Community Health Survey, 23.1% of adult Canadians were obese (body mass index= 30kg/m2) and an additional 36.1% were overweight (body mass index= 25kg/m2). To give perspective on the magnitude of concern this represents six out of every 10 Canadians are overweight or obese (Tjepkema 2005). Abdominal adiposity is associated with cytokine perturbations leading to prothrombotic and proinflammatory states (Grundy2004, Grundy 2008) and these metabolic changes promote cardiometabolic complications (Grundy 2004). To date, body mass index(BMI) has been strongly and positively linked to an increase risk of type 2 diabetes, cardiovascular disease, sleep apnea, osteoarthritis, dyslipidemia, asthma and certain cancers (Fabricatore 2006, NHLBI 1998, Schelbert 2009, Tjepkema 2005).
Aside from increased co-morbidities obese and overweight populations have a decreased life expectancy compared to their normal weight counterparts (Peeters 2003). Despite the significance of this prevalence, an initial weight loss of 5-10% can confer positive improvements in cardiometabolic risk factors regardless of initial BMI (Fabricatore 2006, NHLBI 1998). Dietary intervention is an essential component of a comprehensive weight loss strategy and is considered first line therapy in numerous guidelines (NHLBI 1998). Furthermore, the ideal dietary intervention would not only be effective for weight loss but would also prevent, stabilize or reverse the most common associated comorbidities. A therapeutic lifestyle intervention can be an effective strategy in high risk individuals with coronary heart disease (Gordon 2004). Dietary interventions as they relate to weight loss and the most common comorbidities are the subject of this review.
Regulation of Body Weight and Energy Balance
Daily caloric expenditure depends on three basic elements: basal metabolic rate (BMR), post meal thermogenesis and non-exercise activity thermogenesis. Total caloric expenditure is the sum of an individual’s daily caloric expenditure and exercise induced caloric expenditure. It is well accepted that overall caloric deficiency must be induced for weight loss to occur (Schelbert 2009). Regulation of caloric intake is influenced by the central nervous system. Research is burgeoning in this field and the following neuropeptides have been shown to influence eating behavior by modulating hunger and satiety: vagal stimulation, cholecystokinin, Apolipoprotein A-IV, insulin, PYY, Glucagon-like peptide-1, other glucagonrelated peptides, leptin, gherlin, tumor necrosis factor- α and obestatin (Jensen 2011).
Physiologic Impact of Caloric Deficiency
Dietary caloric restriction antagonizes weight loss efforts by reducing BMR through reductions in thyroid hormones, triiodothyronine (T3) from thyroxine (T4) as well as preferential use of lean muscle mass over adipose tissue for energy. This phenomenon can be mitigated by the inclusion of exercise which favors the maintenance of lean muscle tissue and increases BMR (Jensen 2011).
Dietary Interventions for Weight Loss Caloric Restriction
Caloric restriction is a critical component of successful weight loss (Schelbert 2009). A very low calorie diet (VLCD) is defined as less than 800 kcal/day while a low calorie diet (LCD) is defined as 800-1350kcal/day. A meta-analysis of randomized trials evaluated the efficacy of caloric restriction on short and long term efficacy of weight loss. At the end of six months the average lost was 16.1% and 9.7% of body weight in the VLCD and LCD respectively (Tsai 2006). Despite this initial short statistical difference between the two diets, a greater regain of weight in the VLCD was seen which subsequently equalized the benefits of the diets by one year so that there was no difference in weight loss between the groups (Tsai 2005).
The literature is devoid of studies assessing the long-term metabolic impact of caloric restriction (Kim 2008). A study by Wadden (1990) assessed the influence of caloric restriction influence on thyroid hormones: T3, T4 and reverse T3. Reverse T3 (rT3) is the enzyme responsible for converting T3 (the more active thyroid hormone) to the less active T4. In the VLCD group serum T3 was reduced by 66% while rT3 increased by 27%. When the VLCD group returned to a LCD thyroid function increased but remained 22% lower than baseline at the end of study (Wadden 1990). Further research is needed to better understand if T3 depression and rT3 augmentation effect are temporary or longer term.
Moderate caloric restriction based on estimated total energy expenditure is preferred over VLCD long term. Mild caloric deficiency will result in less antagonizing reflective mechanisms, less thyroid suppression and less BMR suppression. Even with successful weight loss obesity should be viewed as a chronic condition as long-term weight gain is common and should be monitored regularly (Wadden 1993).
Macronutrient Quantity
Many commercial and popular diets tout that their clinical weight loss success is based on a particular combination of carbohydrate, protein and fat. This topic has indeed earned the interest of several investigators.
Low Carbohydrate, High Protein Diet vs. Low Fat, High Carbohydrate Diet
A systematic review analyzed 13 randomized controlled trials that compared low carbohydrate, high protein (LC/HP) ‘ketogenic’ diet to low fat, high carbohydrate (LF/HC) diets. By 12 months a statistically significant difference of 1.05 kg (P <0.05) favored the LC/HP diet (Hession 2009). Despite a statistical significance at 12 months it is questionable whether a modest 1.05 kg difference is of clinical significance at 12 months.
LC/HP Diet vs. LF/HC Diet vs. MedDiet
A two-year prospective trial evaluated three diets head to head. An LC/HP diet according to Atkin’s guidelines, LF/HC diet according to the American Heart Association guidelines and a Mediterranean Diet (MedDiet). The caloric restriction for LF/ HC and MedDiet was 1500 kcal per day for women and 1800 kcal a day for men. The LC/HP diet was restricted based on 20g of carbohydrates per day (Shai 2008).
The greatest amount of weight loss occurred in the first six months for all diet types. At six months, LC/HP showed the most significant weight loss. At the two-year mark, the MedDiet and the Atkin’s diet demonstrated a close to equal average weight loss of 4.4kg and 4.7kg respectively. The LF/HC diet demonstrated inferior weight loss throughout the two-year period with an average 2.9kg of weight loss (Shai 2008). Systematic reviews and prospective studies have consistently reproduced these findings. The statistical differences between the diets are inconsistent at the end of one year. After two years weight regain to some degree is common across all diet types. At two years the LF/HC appears to be inferior to the Mediterranean and LC/HP diet to questionable degree of clinical relevance.
Protein vs. Carbohydrate vs. Fat
A study by Sacks and colleagues (2009) investigated four diet groups based on intakes of carbohydrates, protein and fat. All four groups received the same guidelines for healthy choices of each macronutrient. At six months, 12 months and 24 months there were no significant differences between the four groups regarding weight loss, satiety, hunger and satisfaction with the diet. The greatest weight loss was seen at six months and regain began after 12 months. All diets improved fasting insulin levels and cholesterol panels equally, possibly reflecting a decrease in adiposity and cytokine perturbation rather then the diets (Sacks 2009).
Therefore, from a simple weight loss perspective the optimal diet may be patient dependent since compliance and adherence are the greatest predictors for weight loss (Fabricatore 2006).
“Reduced-calorie diets result in clinically meaningful weight loss regardless of which macronutrients they emphasize (Sacks 2009).”
Impact of Glycemic Index and Glycemic Load on Weight Loss
Glycemic index ranks foods based on the rate that they impact blood sugar levels. Glycemic load is a reflection of the glycemic index plus the total absolute amount of carbohydrates (Wolever 1991). Factors that decrease the glycemic index are the co-ingestion of carbohydrates with fat, protein and/or fiber.
The glycemic index (GI) and glycemic load (GL) of the average North American diet has increased as food-processing advancements and refined carbohydrate intake have risen (Ludwig 2002). High glycemic index/load diets among individuals without diabetes are associated with physiological 24-hour hyperglycemia, hyperinsuliemia, higher C-peptide excretion and higher glycosylated hemoglobin (Hb A1C) concentrations. Homeostatis of glucose are tightly regulated by the endrocrine pancreas via insulin and glucagon. A high glycemic-index meal results in rapid postprandial hyperglycemia leading to reactive hyperinsulinemia. Two to four hours postprandial following a high glycemic meal, mild hypoglycemia occurs inducing hunger and hyperphagia in order re-establish homeostasis. This cycle has metabolic consequences promoting weight gain. Furthermore, this chronic glucotoxicity can lead to β-cell failure and increase the risk of type II diabetes. A low glycemic index meal induces a milder, more prolonged and controlled release of insulin and return to euglycemic state resulting in better glycemic control and satiety (Ludwig 2002).
A randomized controlled trial assessed four diets: high carbohydrate or high protein with low or high GI respectively. Lowering the GI in the high carbohydrate diets resulted in the doubling of fat loss from 2.8kg to 4.5kg in 12 weeks. In the high-protein diets GI did not impact fat loss. In addition, women were more responsive to changes in glycemic index (McMillan- Price 2006). Two Cochrane reviews support low glycemic index/ load meals for both the treatment of obesity (Thomas 2007) and glycemic control of type II diabetes (Thomas 2009).
Critical review of the Cochrane database concluded that there was statistically and significantly greater weight loss in the low glycemic diet (LGD) group as compared to the LF diets. Parameters such as weight loss from fat mass improved as well as satiety. In addition, the resting energy expenditure was not antagonized to the same degree as in the low fat group (Pereira 2004). High GI and GL diets are associated with higher weight gain, fat mass and waist circumference (Hare-Bruun 2006). The limitations of the current research are inconsistent cut-offs between LGD and HGD. This may contribute to some inconsistencies in the literature (Esfahani 2011).
Weight loss can be realized by a degree of caloric deficiency, regardless of macronutrient proportions. Nonetheless, one of the greatest hurdles of weight loss is the very common subsequent weight regain. Typical Western diets induce high glycemic responses that promote postprandial carbohydrate oxidation rather then fat oxidation. This may be a plausible mechanism for the long-term promotion of weight gain. Low glycemic diets support weight control by promoting satiety, maintaining insulin sensitivity and blunting insulin secretion (Brand-Miller 2002).
Dietary Intervention Impact on Mortality and Common Comorbidities
From a simplistic weight loss perspective the review of the literature indicates a slight superiority of the MedDiet and LC/ HP diet over that of the LF/HC. The clinical relevance of these findings is disputable given the negligible magnitude of difference on weight loss. Individuals who are overweight and obese are at increased risk of various comorbidities. Choosing a dietary intervention for weight loss should place a special emphasis on the impact the dietary intervention could have not only on weight loss but also on mortality and common comorbidities.
LF/HC Diet and Cardiometabolic Risk Factors
As reviewed a LF/HC diet has the tendency to be a higher in carbohydrates notably higher simple carbohydrates resulting in an overall higher glycemic index diet. It positively impacts triglyceride to a much lesser degree than both the LC/HP and MedDiet. Furthermore, the LF/HC promotes less glucose control than the Mediterranean Diet (Shai 2008).
HP/LC Diet and Cardiometabolic Risk Factors
A HP/LC diet has been associated with higher mortality from all causes (Trichopoulou 2007), increased risk of renal stone formation, high renal acid load, negative calcium balance and theoretically increased risk for bone loss (Reddy 2002, Fung 2010). While offering benefit relative to a LF/HC diet for the endpoint of weight loss as reviewed above, such a list of complications is concerning. Recommendation of such a strategy for long- term weight maintenance should be done with caution.
MedDiet and Cardiometabolic Risk Factors
The MedDiet has shown positive impact on various health parameters including mood, cognition, erectile function and endothelial function (Féart 2009, Giugliano 2010, Rallidis 2009, Sánchez-Villegas 2009). The MedDiet impacts risk factors such as cholesterol panel improvements as well as reducing the risk of subsequent coronary events (de Lorgeril 2008, Shai 2008).

The MediDiet resulted in a 52% four-year relative risk reduction in the incidence of type II diabetes in high-risk individuals (Salas- Salvadó 2011). With regards to secondary prevention among individuals newly diagnosed with type II diabetes there were 26% fewer individuals started on antihyperglycemics at the end of four years in MedDiet group as compared to the American Diabetic Association diet. We could expect to see much greater impact if the MedDiet was compared to a typical western diet.
Weight loss in general improves cardiometabolic parameters; however, no other diet supports the primary and secondary improvement of hard outcomes such as cardiovascular mortality and all-cause mortality as the MedDiet.
A Low-Glycemic Modified MedDiet, The Future?
A Cochrane review confirmed that glycemic control is improved in a low-glycemic index diet without any increased risk of hypoglycemic events (Thomas 2009). A low glycemic index diet improves glycemic control among individuals with normal glucose control as well as individuals with type II diabetes (Thomas 2009), and improves body composition (Thomas 2007). Combining both the low glycemic diet with MedDiet food composition seems a promising future to synergize their independent benefits.
Adjunctive Consideration on Weight Loss
Several adjunctive treatments have appeared to enhance the results of diets. Adding structure to the diet with menus, recipes and grocery lists improved weight loss (Fabricatore 2009, Heymsfield 2003, Wing 1996) . The added structure of incorporating partial meal replacement has also been shown to produce greater weight loss than a conventional weight loss diet alone (Heymsfield 2003). Non-dietary interventions also play a major role in a comprehensive therapeutic lifestyle intervention. It is beyond the scope of this review to discuss these in any detail but their importance should be noted. Behavioural strategies including cognitive behavioural therapy, motivational interviewing, social support network and exercise regiment synergistically improve adherence, compliance, effectiveness and body composition.
Summary
Modest caloric restriction based on energy expenditure is favored long-term over very low calorie diets. Dietary interventions based on macronutrient proportions alone seem over simplistic and fail to demonstrate any clinically relevant difference in weight loss. Both the MedDiet and a LGD show effective weight loss results as well as important improvements in common comorbidities. A modified low-glycemic MedDiet including smaller more frequent meals, moderate consumption of healthy fat (olive oil), high intake of vegetables and fruit, low quantities of red meat, using poultry and fish to replace beef and lamb, the inclusion of high fiber, and LG whole grains appears to be a desirable intervention strategy given the current state of the literature. The plan must be individualized to the needs of each patient, however, and certain cultural/ religious/ personal preferences may force modification in order to maximize long term compliance. Obesity must be viewed as a chronic condition since weight gain is common. A maintenance dietary program, continual support and behavioural strategies are critical for long-term success.
Reference:
Brand-Miller JC, Holt SHA, Pawlak DB, McMillan J. Glycemic index and obesity. Am J Clin Nutr. 2002 Jul:76(1):281S–5S.
de Lorgeril M, Salen P. The Mediterranean diet: rationale and evidence for it benefit. Curr Atheroscler Rep. 2008 Dec;10(6):518–522.
Esfahani A, Wong JMW, Mirrahimi A, Villa CR, Kendall CWC. The application of the glycemic index and glycemic load in weight loss: A review of the clinical evidence. IUBMB Life. 2011 Jan;63(1):7–13.
Fabricatore AN, Wadden TA. Obesity. Annu Rev Clin Psychol. 2006;2:357–377.
Féart C, Samieri C, Rondeau V, Amieva H, Portet F, Dartigues JF, Scarmeas N, Barberger-Gateau P. Adherence to a Mediterranean diet, cognitive decline, and risk of dementia. JAMA. 2009 Aug;302(6):638–648.
Fung TT, van Dam RM, Hankinson SE, Stampfer M, Willett WC, Hu FB. Lowcarbohydrate diets and all-cause and cause-specific mortality: Two cohort Studies. Ann Intern Med. NIH Public Access, 2010 Sep;153(5):289–298.
Giugliano F, Maiorino MI, Bellastella G, Autorino R, De Sio M, Giugliano D, Esposito K. Adherence to Mediterranean diet and erectile dysfunction in men with type 2 diabetes. J Sex Med. 2010 May;7(5):1911–1917.
Gordon NF, Salmon RD, Franklin BA, Sperling LS, Hall L, Leighton RF, Haskell WL. Effectiveness of therapeutic lifestyle changes in patients with hypertension, hyperlipidemia, and/or hyperglycemia. AJC. 2004 Dec;94(12):1558–1561.
Grundy SM. Definition of Metabolic Syndrome Report of the National Heart, Lung, and Blood Institute/American Heart Association Conference on Scientific Issues Related to Definition. Circulation. 2004 Jan:109(3);433-8.
Grundy SM. Promise of low-density lipoprotein-lowering therapy for primary and secondary prevention. Circulation. 2008 Jan;117(4):560–8; discussion 573.
Hare-Bruun H, Flint A, Heitmann BL. Glycemic index and glycemic load in relation to changes in body weight, body fat distribution, and body composition in adult Danes. Am J Clin Nutr. 2006 Oct;84(4):871–9; quiz 952–3.
Hession M, Rolland C, Kulkarni U, Wise A, Broom J. Systematic review of randomized controlled trials of low-carbohydrate vs. low-fat/low-calorie diets in the management of obesity and its comorbidities. Obes Rev. 2009; Jan 10(1):36–50.
Heymsfield SB, van Mierlo CAJ, van der Knaap HCM, Heo M, Frier HI. Weight management using a meal replacement strategy: meta and pooling analysis from six studies. Int J Obes Relat Metab Disord. 2003 May;27(5):537–549.
Jensen MD. 227 – Obesity, in:, Goldman’s Cecil Medicine. Elsevier Inc., 2011 pp. 1409–e227–1.
Kim B. Thyroid hormone as a determinant of energy expenditure and the basal metabolic rate. Thyroid. 2008 Feb;18(2):141–144.
Ludwig DS. The Glycemic Index: Physiological Mechanisms Relating to Obesity, Diabetes, and Cardiovascular Disease. JAMA: The Journal of the American Medical Association. 2002 May; 287(18):2414–2423.
McMillan-Price J, Petocz P, Atkinson F, O’neill K, Samman S, Steinbeck K, Caterson I, Brand-Miller J. Comparison of 4 diets of varying glycemic load on weight loss and cardiovascular risk reduction in overweight and obese young adults: a randomized controlled trial. Arch Intern Med. 2006 July;166(14):1466–1475.
NHLBI, Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults: the evidence report. 1998.
Peeters A, Barendregt JJ, Willekens F, Mackenbach JP, Mamun AlA, Bonneux L, NEDCOM. Obesity in adulthood and its consequences for life expectancy: a life-table analysis. Ann Intern Med. 2003;138(1):24–32.
Pereira MA. Effects of a Low-Glycemic Load Diet on Resting Energy Expenditure and Heart Disease Risk Factors During Weight Loss. JAMA. 2004;292(20): 2482–2490.
Rallidis, LS, Lekakis, J, Kolomvotsou, A, Zampelas, A, Vamvakou, G, Efstathiou, S, Dimitriadis G, Raptis SA, Kremastinos DT. Close adherence to a Mediterranean diet improves endothelial function in subjects with abdominal obesity. Am J Clin Nutr. 2009;90(2):263–268.
Reddy ST, Wang CY, Sakhaee K, Brinkley L, Pak CYC. Effect of low-carbohydrate high-protein diets on acid-base balance, stone-forming propensity, and calcium metabolism. Am J Kidney Dis. 2002;40(2):265–274.
Sacks FM, Bray GA, Carey VJ, Smith SR, Ryan DH, Anton SD, McManus K, Champagne CM, Bishop LM, Laranjo N, Leboff MS, Rood JC, de Jonge L, Greenway FL, Loria CM, Obarzanek E, Williamson DA. Comparison of weight-loss diets with different compositions of fat, protein, and carbohydrates. N Engl J Med. 2009;360(9): 859–873.
Salas-Salvadó J, Bulló M, Babio N, Martínez-González MA, Ibarrola-Jurado N, Basora J, Estruch R, Covas MI, Corella D, Arós F, Ruiz-Gutiérrez V, Ros E, PREDIMED Study Investigators, Reduction in the incidence of type 2 diabetes with the Mediterranean diet: results of the PREDIMED-Reus nutrition intervention randomized trial. Diabetes Care. 2011 Jan;34(1):14–19.
Sánchez-Villegas A, Delgado-Rodríguez M, Alonso A, Schlatter J, Lahortiga F, Serra-Majem L, Martínez-González MA. Association of the Mediterranean dietary pattern with the incidence of depression: the Seguimiento Universidad de Navarra/University of Navarra follow-up (SUN) cohort. Arch Gen Psychiatry. 2009 Oct;66(10):1090–1098.
Schelbert. Comorbidities of Obesity. Primary Care Clinics in Office Practice. 2009 Sep;36(2):271–285.
Shai I, Schwarzfuchs D, Henkin Y, Shahar DR, Witkow S, Greenberg I, Golan R, Fraser D, Bolotin A, Vardi H, Tangi-Rozental O, Zuk-Ramot R, Sarusi B, Brickner D, Schwartz Z, Sheiner E, Marko R, Katorza E, Thiery J, Fiedler GM, Blüher M, Stumvoll M, Stampfer MJ, Dietary Intervention Randomized Controlled Trial DIRECT Group, 2008. Weight loss with a low-carbohydrate, Mediterranean, or lowfat diet. N. Engl. J. Med. 2008 Jul;359(3):229–241.
Thomas D, Elliott EJ. 2009. Low glycaemic index, or low glycaemic load, diets for diabetes mellitus. The Cochrane Library. John Wiley & Sons, Ltd, Chichester, UK, 2009 Jan;(1), CD006296.
Thomas D, Elliott EJ, Baur L. Low glycaemic index or low glycaemic load diets for overweight and obesity. Cochrane Database of Systematic Reviews. John Wiley & Sons, Ltd, Chichester, UK, 2007; Sep(3), CD005105.
Tjepkema M. Canada, S., Nutrition: Findings from the Canadian Community Health Survey – Adult Obesity in Canada: Measured height and weight. 2005 Jul:1–32.
Trichopoulou A, Psaltopoulou T, Orfanos P, Hsieh CC, Trichopoulos D. Lowcarbohydrate- high-protein diet and long-term survival in a general population cohort. Eur J Clin Nutr. 2007 May;61(5):575–581.
Tsai AG, Wadden TA. Systematic review: an evaluation of major commercial weight loss programs in the United States. Ann Intern Med. 2005 Jan;142(1):56–66.
Tsai AG, Wadden TA. The evolution of very-low-calorie diets: an update and metaanalysis. Obesity (Silver Spring). 2006 Aug;14(8):1283–1293.
Wadden T. Treatment of Obesity by Moderate and Severe Caloric Restriction: Results of Clinical Research Trials. Ann Intern Med. 1993:119(7pt2):688-693.
Wadden TA, Mason G, Foster GD, Stunkard AJ, Prange AJ,. Effects of a very low calorie diet on weight, thyroid hormones and mood. Int J Obes Relat Metab Disord. 1990 Mar;14(3):249–258.
WHO 2002. The World Health Report 2002. WHO. 2002. 1–230.
Wing RR. Food provision vs structured meal plans in the behavioural treatment of obesity. Int J Obes Relat Metab Disord. 1996. 20(1), 55-62
Wolever TM, Jenkins DJ, Jenkins AL, Josse RG. The glycemic index: methodology and clinical implications. Am J Clin Nutr. 1991 Jul;54(5):846–854.
Endocrine Disruptors

Endocrine Disruptors
Abstract:
It can be hypothesized that the ingestion of endocrine disruptor (ED) metabolites (from the water supply and food chain) can result in detrimental outcomes for males and females, such as prostate and breast cancer, infertility and C-sections; either through mechanisms of hormonal imbalance or dysfunctional metabolism. Physiological and biological mechanisms of action thought to be involved include creation of a state of estrogen dominance, and that EDs can alter the morphology and function of sperm and the estrogen receptor. Although further evidence is needed to establish causation between an increased use of the BCP, a high level of metabolites in the water supply, and an increasing number of reproductive diseases, the alarming patterns between these variables warrant additional study.
CONCERNS ABOUT ENDOCRINE DISRUPTORS IN THE WATER SUPPLY AND BIOACCUMULATION
Endocrine disruptors, although detrimental on their own, are not the only concern; there is a) a lack of consistent measurement standards of ED metabolites in the water supply, b) variability in the efficiency of methods that extract EDs and c) a lack of published evidence to link bioaccumulation of reproductive specific metabolites to human disease. Primarily, there is little formal regulation involving monitoring of pharmaceutical metabolites in regional water supplies. Additionally, several countries do not have legislation in place for continuous follow up of these specific chemicals. This variability is also present in treatment facilities. Processes in treatment plants have demonstrated varying removal rates for pharmaceuticals, ranging from less than 20% to greater than 90% (WHO 2011). A report by the International Joint Commission in Windsor showed that pharmaceutical metabolites can exert detrimental effects, such as alterations in the reproductive system of aquatic organisms and humans. Bioaccumulation of EDs has been demonstrated in various environmental compartments, however, their pathological endpoints have not been fully investigated, nor their causative chemical metabolites fully regulated in the United States and Canada (Kemp 2011).
An endocrine disruptor is defined as any natural or synthetic metabolite or compound that alters hormones, enzymes or receptors within the body. Endocrine disruptors can be classified into several categories, two of which will be addressed in this review: a) chemical toxins, and b) pharmaceutical metabolites.
Endocrine Disruptors: Chemical Metabolites
There are several types of toxin related endocrine disruptors, such as polychlorinated biphenyls (PCB), polyvinyl chlorides (PVC), pthalates and parabens that have been correlated with hormonal dysfunction. Bisphenol A (BPA), furans, polybrominated diphenyl ethers (PDBE) and dioxins are well known carcinogens (Kaur 2005). Organochlorines resist biochemical breakdown, have a long half life and also accumulate as EDs in the environment (Fisher 1999).
Food sample analysis in Spain, the USA, and Japan have collectively shown ED levels from 340-3000 parts per trillion (ppt) and have confirmed that all foods containing animal fats had PBDE by-products (Schuhmacher 2007, Seely 2007). It has been estimated that the daily human intake of PBDEs is approximately 0.51 nanograms (Ramos 2006). Further evidence of bioaccumulation was shown in patient fat biopsies that were chemically analyzed following exposure to polychlorinated dioxins, furans and PCBs. Levels of hepta- and octachlorinated furans and dioxins of up to 8400 parts per trillion (ppt) were found in one repeatedly exposed person in comparison to the fat from control group members (from patients with no overtly known exposure to furans or dioxins) that were several 100 ppt (Schecter 1985).
Endocrine Disruptors: Pharmaceutical Metabolites
In addition to toxins, pharmaceutical metabolites accumulate in the water supply and contribute towards physiological dysfunction. These include but are not limited to ethinyl estradiol (EE2), levonorgestrel (LNG) and norethindrone (NET). EE2 is one of the main metabolites of oral contraception, and is also administered as patches, injections and rings. EE2 is more chemically active than other estrogenic metabolites. It is not the largest contributor to estrogen in the water supply, however it has joined other synthetic estrogens, such as those from dairy cows, fertilizers and industrial chemicals (Moore 2011).
There are numerous studies that identify how contraceptives are: a) found in the water supply, and b) pose health hazards to wildlife and other species in the food chain. The Songhua River and Harbin drinking water study charted the removal rates of estrogenic activity, which was 34.6% to 50.5% in Harbin, and revealed that estrogenic pollutants in source water were not efficiently removed in treatment plants (Shao 2009). The Endocrine Society released a statement that low level, chronic exposure to environmental endocrine disruptors has caused or contributed to adverse human health effects (Diamanti-Kandarakis 2009). A collective of in vitro, animal and a few human studies has provided compelling evidence that exposures to either birth control pill (BCP) or estrogen metabolites through the water supply had biological consequences. This has been corroborated by the discovery of inter sex fish near sewage plants in various parts of the world, such as the U.S.A, Europe and Japan (Iwanowicz 2009, Jobling 2004). Another interesting animal study showed that chronic exposure to levonorgestrel (LNG) caused oxidative stress to Dreissena polymorpha (Contardo- Jara 2011). A human study showed that an insecticide altered sperm function by altered membrane depolarization and membrane dipole potential; this lowered water molecular dynamics in the superior part of the external membrane (Silvestroni 1997). It should be noted, however, that unlike other chemical toxic metabolites, comprehensive evidence of quantified bioaccumulation of BCP metabolites in humans is lacking to date.
TRENDS IN ENDOCRINE DISRUPTOR LEVELS AND GENITOURINARY DISEASE Increased Use of the Birth Control Pill
There has been a rise in the utilization of contraception, more specifically an overall trending to an increased use of the birth control pill (BCP) through recent decades (Moore 2011). The BCP was released into the Canadian market 50 years ago. The Canadian Contraception Study determined that 84 % of Canadian women use or have used the BCP (Fisher 2002, O’Malley 2001). Eighty three percent of the “effluent” sewage samples had EE2 from the BCP (0.07 to 2.6 ng/L); and induced estrogenic responses in fish (Tyler 2009).
There is an average daily dose range of 30 to 35 μg to 1 mg of EE2/ pill. Human urine is the major source of natural and synthetic estrogens in the water supply (Wise 2010). Of the 38.2 million women in the USA using contraception in 2006–2008, the pill accounts for about 28% of contraceptive users, and the percent of women aged 15-44 currently using the pill is 17% (Martinez 2012).
The Use of the Birth Control Pill and Reproductive Cancers
There is direct evidence for an increased risk of breast and cervical cancers with the use of BCPs (Burkman 2004). Several studies including but not limited to a 2003 analysis by the International Agency for Research on Cancer (IARC) and a systematic review by Lancet found an increased risk of cervical cancer with longer use of BCPs (Moreno 2002, Smith 2003). The results from a breast cancer study showed that the highest risk was found in women aged 20-34, who used BCPs within 5 years prior to diagnosis of disease (Althuis 2003). Evidence for indirect risk (through ingestion of BCP related EDs through the water supply) of reproductive female cancers is lacking, although intriguing patterns have been published for male cancers.
Male reproductive diagnoses, such as prostate cancer have recently been etiologically investigated. It was theorized that BCPs were excreted in the urine and travelled into the water supply; concurrently, scientific findings have suggested that low levels may cause cancer, including prostate cancer (Ubelacker 2011). They further postulated that in countries where BCP use was higher, prostate cancer had a greater incidence. A more recent study showed that BCP use was significantly associated with prostate cancer incidence and mortality in the individual nations worldwide (r=0.53), respectively; p<0.05 for all) and with BCP use in Europe (r=0.545, p<0.05), whereas other contraceptives did not correlate with prostate cancer incidence nor mortality (Margel 2011). Although these findings do not necessarily infer causation, these aligning trends should not be ignored, and further studies are warranted.
The Impact of Endocrine Disruptors on Infertility and Caesarean Sections
Recent human studies have elucidated that decreasing fertility could be due to environmental toxic metabolites; biochemically (hormones) or molecularly (cell interactions). One study in males from an infertility clinic demonstrated that an elevation in urinary BPA concentration was associated with decreases in sperm concentration, motility, and morphology of 23% (95%CI -40%, -0.3%), 7.5% (-17%, +1.5%), and 13% (-26%, -0.1%), respectively; this was also associated with a 10% (0.03%, 19%) increase in sperm DNA damage (Meeker 2010). A study of female exposure to the chemical pentachlorophenol, utilized as a lumber preservative, showed altered hypothalamic activity, and was thought to cause low level impaired ovarian function and hormonal insufficiency (Gerhard 1999).
There has also been a notable increase in Caesarean sections (C-section) in recent decades. The Canadian Institute for Health Information stated that the C-section rate has risen; up to 26% of babies born in hospitals in 2005, compared to 23% five years earlier and 17% in 1993 (Hall 2009). Some of the causes can be attributed to technological intervention, position of labour and birth complications; however, chemical causes through bioaccumulation may have been overlooked. Estrogen induces labour by increasing the expression of pro-contraction genes in cells of the myometrium around the time of delivery. The induction of contraction-related gene expression is modulated by signalling outside the nucleus (ERK/MAP) through the estrogen receptor (ER)α (Welsh 2011). Therefore, it can be postulated that dysfunctional estrogen metabolism, signalling and concentration that are caused by synthetic estrogens from ED could result in changes in labour patterns. Several mechanisms can be hypothesized: a) synthetic estrogens may not stimulate the ER with affinity that is sufficient to upregulate signalling, b) high levels of EDs in humans over time may downregulate the estrogen receptor by number or potency, and c) reactive oxygen species from ED accumulation may result in altered gene expression/protein production. Although published evidence between ED bioaccumulation in humans and rates of C-sections is lacking, the putative link and associated mechanisms of action deserve consideration.
RELEVANT BIOCHEMICAL AND MOLECULAR MECHANISMS OF ACTION
Hormone Metabolism
The release of EDs into the water supply is thought to create a state of estrogen dominance (associated with cancer, fibroids and endometriosis). Estrogen (comprised of 17 carbons), is hydroxylated at either C2, C4 or C16 positions; C4 and C16 are thought to be activated by EDs and are associated with breast cancer (Kabat 1997). Hormonal dysfunction is also seen in male reproductive hormones; studies have confirmed inverse associations between ED concentrations and testosterone levels (Meeker 2010).
Infertility
The mechanisms of action by which ED may cause male infertility consist of altered sperm count, altered quality of semen, dysfunctional cell signalling and DNA damage. A reduction in the sperm count and quality can be attributed to PI3K/c-Src/FAK and MAPK signalling on a molecular level, and anatomically, a destruction of cellular junctions by reactive oxygen species (Wong 2011). Regarding mechanisms of female infertility, the binding of EDs to the ER and activation of secondary messenger kinases, as well as calcium influx are at play (Robins 2011). During pregnancy, ED’s may alter meiotic spindle formation (Fujimoto 2011).
CONCLUSION
Although there is an overall lack of causal evidence linking estrogenic metabolites from birth control pills to reproductive diagnoses, there are critical trends and disease patterns identified: increased use of the birth control pill in recent decades, a rise in male and female reproductive cancers, infertility and caesarean sections. More importantly, it may be too early to witness the full effects of increased EDs in the water supply at this point in time, as a critical threshold concentration for detrimental effects may not have been reached for some diseases. Bioaccumulation may dredge up these detrimental effects over time. This principle is evident from the rise in the incidence of various cancers across the globe today that are thought to originate from exposures to toxins in previous decades. Research must include a focus on the past and the future, rather than waiting for the tipping point at present; observation should include searching the past for patterns and trends that may allude to disease incidence, and looking to the future to anticipate prophylactic strategies of modulating chemical toxins and pharmaceutical metabolites in the environment.
References
Althuis MD, Brogan DD, Coates RJ, Daling JR, Gammon MD, Malone KE, Schoenberg JB, Brinton LA. Breast Cancer in Very Young Pre-menopausal Women (United States). Cancer. 2003; 14(2):151-60
Burkman, R, Schlesselman JJ, Zieman M. Safety concerns and health benefits associated with oral contraception. American Journal of Obstetrics and Gynecology. 2004; 190 (4 Suppl.):S5-22.
Contardo-Jara, V, Lorenz C, Pflugmacher S, Nützmann G, Kloas W, Wiegand C. Molecular effects and bioaccumulation of levonorgestrel in the non-target organism Dreissena polymorpha. Envirn Pollut. 2011; 159 (1): 38-44.
Diamanti-Kandarakis, E, Bourguignon, JP, Giudice LC, Hauser R, Prins GS, Soto AM, Zoeller RT, Gore AC. Endocrine-disrupting chemicals: an Endocrine Society scientific statement. Endocrine Rev. 2009; 30 (4): 293-342.
Fisher, BE. Most unwanted persistent organic pollutants. Envir Health Perspect. 1999; 107 (1): A18-23.
Fisher W, Boroditsky, R, and B, Morris. The 2002 Canadian Contraception Study: Part 1.Womens Health. 2002; (1): 1-22
Fujimoto VY, Kim D, vom Saal FS, Lamb JD, Taylor JA, Bloom MS. Serum unconjugated bisphenol A concentrations in women may adversely influence oocyte quality during in vitro fertilization. Fertil Steril. 2011; 95(5):1816-9.
Gerhard, I, Frick A, Monga B, Runnebaum B. Pentachlorophenol exposure in women with gynecological and endocrine dysfunction. Environ Res. 1999; 80(4): 383-8.
Hall, J. What is behind Canada`s C section rate? Research and Innovation, University of Toronto 1 Oct 2009; epub.
Iwanowicz, LR, Blazer VS, McCormick SD, Vanveld PA, Ottinger CA. Aroclor 1248 exposure leads to immunomodulation, decreased disease resistance and endocrine disruption in the brown bullhead, Ameiurus nebulosus. Aquat Toxicol. 2009; 93 (1): 70-82.
Jobling, S, Casey D, Rogers-Gray T, Oehlmann J, Schulte-Oehlmann U, Pawlowski S, Baunbeck T, Turner AP, Tyler CR. Diamanti-Kandarakis E, Bourguignon JP, Giudice LC, Hauser R, Prins GS, Soto AM, Zoeller RT, Gore AC. Comparative responses of molluscs and fish to environmental estrogens and an estrogenic effluent. Aquat Toxicol. 2004; 66 (2): 207-22.
Kabat, GC et al., Urinary estrogen metabolites and breast cancer: a case-control study. Cancer Epidemiol Biomarkers Prev. 1997; 6 (7): 505-9.
Kaur, SD,. The Complete Natural Medicine Guide to Women’s Health. Toronto: Robert Rose Inc., 2005.
Kemp, Brian. 5 Chemical Threats to the Great Lakes. CBC News. 22 Sep 2011: website link. http://www.cbc.ca/news/canada/windsor/story/2011/09/21/great-lakesthreat- list.html
Margel, D, Fleshner NE. Oral contraceptive use is associated with prostate cancer: an ecological study. BMJ. 2011; 1(2) e000311.
Martinez, G, Daniels, K and A Chandra. National Health Statistics Report No.51: Fertility of Men and Women Aged 15–44 Years in the United States: National Survey of Family Growth, 2006–2010.2012; (51): 1-29.
Meeker, JD. Exposure to environmental endocrine disrupting compounds and men’s health. Maturitas 2010; 66 (3): 236-41.
Meeker, JD, Ehrlich S, Toth TL, Wright DL, Calafat AM, Trisini AT, Ye X, Hauser R. Semen quality and sperm DNA damage in relation to urinary bisphenol A among men from an infertility clinic. Reprod Toxicl. 2010; 30 (4): 532-9.
Moore, K, McGuire KI, Gordon R, Woodruff TJ. Birth control hormones in water: separating myth from fact. Contraception. 2011; 84 (2): 115-8.
Moreno, V, Bosch FX, Munoz N, et al. Effect of oral contraceptives on risk of cervical cancer in women with human papillomavirus infection: The IARC multicentric case-control study. Lancet. 2002; 359 (9312) 1085-1092.
O’Malley, Martin, Wood, O and Amy Foulkes. The Birth Control Pill. CBC News-In Depth: Genetics and Reproduction. 3 Jul 2001.
Ramos, JJ, Gomara B, Fernandez MA, Gonzalez MJ. A simple and fast method for the simultaneous determination of polychlorinated biphenyls and polybrominated diphenyl ethers in small volumes of human serum. J Chromatogr. 2006; 1152 (1-2): 124-9.
Robins JC, Marsit CJ, Padbury JF, Sharma SS. Endocrine disruptors, environmental oxygen, epigenetics and pregnancy. Front Biosci (Elite Ed). 2011; (3):690-700.
Schecter, A, et al. Patient fat biopsies for chemical analysis and liver biopsies for ultrastructural characterization after exposure to polychlorinated dioxins, furans and PCBs. Environmental Health Perspectives. 1985; (60): 241-254.
Schuhmacher, M, Kiviranta H, Vartiainen T, Domingo JL. Concentrations of polychlorinated biphenyls and polybrominated diphenyl ethers in milk of women from Catalonia, Spain. Chemosphere. 2007; 67 (9): S295-300.
Seely D, Fernandes R, Young S. Flame Retardants and Cancer Risk. Encyclopedia of Cancer and Society, edited by Graham A. Colditz. Thousand Oaks, CA: Sage Publications. 2007; (3):1190.
Shao, XL, Wen G, Ma J. Survey of estrogenic activity of Songhua River water and drinking water of Harbin. Juan Xing Ke Xue. 2009; 30 (5): 1362-7.
Silvestroni, L, Fiorini R, Palleschi S. Iwanowicz LR, Blazer VS, McCormick SD, Vanveld PA, Ottinger CA. Partition of organochlorine insecticide lindane into the human sperm surface induces membrane depolarization and Ca2+ influx. Biochem. 1997; 321 (pt3) 691-8.
Smith, JS, Green J, Berrington de GA, et al., Cervical cancer and use of hormonal contraceptives: A systematic review. Lancet. 2003; 361 (9364):1159-1167.
Tyler, C. R., et al. Environmental Health Impacts of Equine Estrogens derived from Hormone Replacement Therapy. Environ Sci Technol. 2009; 43 (10): 3897-3904.
Ubelacker, Sheryl. Is the Pill behind rising prostate cancer rates? The Globe and Mail 14 Nov 2011; online.
Welsh, T, Johnson M, Yi L, Tan H, Rahman R, Merlino A, Zakar T, Mesiano S. Estrogen Receptor Expression and Function in the Pregnant Human Myometrium: Estradiol via Estrogen Receptor- Activates ERK1/2 Signaling in Term Myometrium.” J Endocrinol. 2011; 212 (2): 227-38.
WHO. Pharmaceuticals in drinking water. Public Health Report. Geneva. WHO Press. 2011. http://www.who.int/water_sanitation_health/publications/2011/ pharmaceuticals_20110601.pdf
Wise, A, O’Brien K, Woodruff T. Are oral contraceptives a significant contributor to the estrogenicity of drinking water? Environ Sci Technol. 2011; 45 (1): 51-60.
Wong, EW, Cheng CY. Impacts of environmental toxicants on male reproductive dysfunction. Trends Pharmacol Sci. 2011; 32 (5): 290-9.
Chronic Venous Insuffi ciency (CVI)

Chronic Venous Insuffi ciency (CVI)
Integrative management approaches
Abstract
Chronic venous insuffi ciency (CVI), also known as varicose vein disease, is seen with comorbid conditions of ischemic heart disease, type II diabetes, and obesity which are growing in the Western world and as such the management and support of CVI is a necessity. Hallmark infl ammation and edema in the extremities in CVI is moderately well-managed to date with compression stockings and diuretics in conventional therapy. Recent exploration of the role of reactive oxygen species at the cellular level elucidates more causal reasons for this infl ammation and edema. Antioxidant therapies, protective nitric oxide supplied through acupuncture, dietary modifi cation in addition to herbal supports such as diosmin, hespiridin, and horse chestnut provide exciting future avenues for research of the maintenance and slowing of tissue damage in individuals with CVI.
Varicose vein disease, or chronic venous insuffi ciency (CVI), is a common health condition, aff ecting up to 65% of women and 50% of men over the age of 45, and accompanied by comorbidities of cardiovascular disease, type II diabetes, and obesity (Bergan 2006, Burkett 1973, McLaff erty 2008, Robertson 2008). Collapsed venous valves lead to pooled venous fl uid in tissues, inducing infl ammation that progresses to signifi cant tissue damage. To date, the etiology of this process has not been well elucidated. In recent years, however, the endothelial dysfunction of CVI has been viewed as related not only to the eff ects of long-term infl ammation but also to oxidative stress and a decreased capacity for antioxidant defence (Carrasco 2009). More rigorous identifi cation of herbal anti-infl ammatory supports for vascular dysfunction as well as the use of antioxidant-enhancing mechanisms such as acupuncture and L-arginine has made the role of complementary supports for CVI a more mainstream option for treatment in coming years.
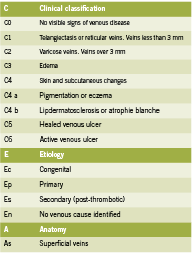
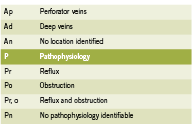
Attempts to properly organize CVI symptomatology lead to the development of the CEAP rubric in 1995. Since tested for its consistency, the CEAP acronym organizes CVI by clinical (C), etiological (E), anatomical (A) and physiological (P) condition states (Porter 1995) and has been proven to be the best objective manner of testing and classifying CVI between patients and clinicians (Kistner 1996). Table 1 outlines the classifi cations for CEAP.
Common conventional treatments include compression therapy and sclerotherapy, with compression therapy the current gold standard (Braunwald 2001). Compression therapy (including specialized stockings; “TEDS”) provides mechanical support to minimize fl uid pooling and maximize limb function in patients with progressed disease.
e progression of CVI is characterized by infl ammatory mediators that cause collagen & elastin remodelling in the endothelium, and this results in loss of vessel wall integrity. is remodelling, coupled with ongoing infl ammation and reactive oxygen species production leads to vein collapse (Raff etto 2008). Vasorelaxation responses that are controlled by norepinephrine, acetylcholine, and serotonin dynamics are all decreased in individuals with CVI (Belcaro 1989, Belcaro 1988, Georgescu 2009).
Reactive oxygen species (ROS) play a key role in mediating chronic infl ammation; ROS cause oxidation of lipid membranes (Guzik 2011), and DNA damage that further amplifi es the infl ammatory response (Halliwell 2000). ROS are reactive chemical forms of oxygen that include superoxide anions (O2-) and hydroxyl radicals that are capable of damaging cells. Antioxidant mechanisms like the enzyme superoxide dismutase can minimize this damage by producing hydrogen peroxide (H2O2) from the superoxide anion (O2-) which will then be converted by catalase to water. However, in enzymatic defi ciency and infl ammation, superoxide anions can go “unchecked” by normal antioxidant mechanisms. Additionally, the enzymes NAD(P)H oxidase, cyclooxygenase, nitric oxide synthase, and xanthine oxidase can all form superoxide radicals (O2-) from molecular oxygen (O2), enhancing the problem (Halliwell 2000, Klaubunde 2012, Krzysciak 2011).
Produced by L-arginine reacting with nitric oxide synthase, NO is protective to the endothelium (Meletis 2006). Increased NO and its metabolites cause an increase in guanylate cyclase (GC) and cGMP, which leads to relaxation of vascular smooth muscle and vasodilation (Ignarro 1990, Ignarro 1993, Klaubunde 2012, Meletis 2006). NO is also anti-infl ammatory and anti-thrombotic as it discourages platelet aggregation in the endothelium and pro-inflammatory mediators. The presence of superoxide anion scavenges NO, reducing its bioavailability leading to vasoconstriction, increased leukocyte-endothelial adhesion through intracellular adhesion molecules (ICAM), and structural blood vessel changes contributing to vein collapse. Indeed, decreased nitric oxide (NO) is seen in atherosclerosis, type II diabetes, hypertension, and smoking (Guzik 2002). Inflammation causes more fluid to be drawn into the collapsed venous systems, exacerbating the condition (Krzyściak 2011, Yasim 2008). Hence, antioxidant therapy to support NO production is beneficial for CVI, as is management of inflammation to decrease immunemediated DNA destruction.
Integrative Treatments for Oxidative Stress with CVI
Acupuncture is a therapy that offers a multitude of beneficial effects for CVI. Acupuncture has proven to have analgesic effects via stimulation of alpha, delta and C-fibres in the skin and muscles responsible for pain perception; these fibres initiate cascades inducing peripheral vasodilation and production of proinflammatory agents such as substance P, opioids, somatostatin, and vasoactive intestinal peptide. As a result, acupuncture has the ability to influence fluid movement and edema in tissues (Cassileth 2011, Lewith 1983, Ma 2003, Sprott 1998). It is believed that acupuncture meridians and points themselves are regions of low electrical resistance and high electrical conductivity in the nervous system, and as a result may be able to impact the sympathetic nervous system, the release of substance P, and decreased pain perception (Ahu 1981, Ma 1993, Zhu 1989).
An increased presence of NO has been found in skin areas where acupuncture meridians are found, as well as generally increased NO levels in the skin following acupuncture in vitro and in vivo in both human and animal models (Li 2003, Ma 2003). Twenty subjects with hand and forearm pain were exposed to two minutes of either acupuncture at the points LI 4, P6, P8, L6, and H5 or non-invasive sham acupuncture for the same length of time. Non-sham acupuncture sessions were found to have significantly increased blood flow around the chosen points both five and 60 minutes following the session, as well as increasing blood NO concentration (Tchiyua 2007). In other studies, however, sham acupuncture has also been found to have blood flow increasing effects, and further studies will be needed to understand the NO-enhancing capacity of standard acupuncture to truly distinguish between placebo effects (Lewith 1983, Park 2011, Takakura 2011,). A case report exists of a 69-year old male with bilateral venous ulcers and rheumatoid arthritis who was treated with compression bandages and an anti-inflammatory regime (NSAIDS, sulfasalazine, methotrexate), but without adequate healing; when treated with three weekly sessions of acupuncture at points ST36, KI3 and LR3 bilaterally, full healing of the ulcer on the left leg was seen within three weeks (Mears 2003). Since compression therapy is the current most utilized treatment for CVI, a larger study is being conducted to compare acupuncture with compression bandages (Vas 2011).
Botanical Agents
Horse chestnut seed extract (HCSE) has been used widely in Europe for many years for CVI, hemorrhoids, and post-operative edema, and is slowly being recognized for these purposes in North America (Tiffany 2002, Sirtori 2001). Aescins, a combination of triterpene saponins from horsechestnut, are believed to be responsible for reducing the small vessel permeability of the venous system (Ulbricht 2002). Horsechestnut also contains anti-inflammatory bioflavonoids (quercitin and kaempferol), proanthocyanidin A2, and venotonic coumarins (fraxin and aesculin) (Tiffany 2002, Lorenz 1960, Mrwa 1986). HCSE’s are typically standardized to contain 16-20 percent aescin, and the oral dosage is typically 100-150 mg aescin/day in divided doses as a dried seed or 2-3 mL daily as a tincture (Abascal 2007, Tiffany 2002). HSCE cannot be used in those with kidney disease or broken skin due to irritating effects (Abascal 2007).
On a molecular level, HCSE is thought to act by increasing sensitization to calcium ions, thus decreasing permeability of small vessels and enhancing venous contractile activity which decreases edema (Tiffany 2002). Its immune-stabilizing properties include the ability to decrease leukocyte migration and adherence, and reduce local levels of inflammatory mediators (Pangieri 1992). Systematic reviews of RCTs investigating HCSE have been conducted, with the most recent in 2006 (Pittler 2004, Pittler 2006). Pittler concluded that HCSE treatment was associated with a significant improvement in CVI symptoms of leg pain, itching, and fatigue, as well as reduction in lower-leg volume as a short-term treatment (2006). RCTs have also compared HCSE with compression therapy. Ottillinger and Greeske found that both therapies were equally effective in earlier stages of CVI, when irreparable damage has not occurred in the venous system; however in later stages of CVI, only compression therapy was effective compared to placebo (p <0.001), whereas HCSE was not (p = 0.115) (Diehm 1996, Ottillinger 2001). Further research needs to be done to determine the clinical stages in which HSCE is best administered.
Diosmin and hespiridin are bioflavonoids used for CVI, and have been patented as Daflon ® or a micronized purified flavonoid fraction (MPFF). Danielsson (2002) compared 101 patients randomised to either MPFF twice daily (Daflon ® 500 mg, standardized as 90% diosmin and 10% flavonoids expressed as hesperidin) or placebo for 60 days. Evaluation was with CEAP (subjective symptoms of pain, edema, fatigue rated from 1-3 by patients), plethysmography (foot-volumetry), and duplexultrasonography before and after the treatments. Night cramps were significantly improved (p=0.03) with MPFF compared with placebo; however there was no significant effect on tiredness, heaviness, pain, and swelling as well as duplex-ultrasonography compared to placebo (Danielsson 2002).
Pycnogenol, a French maritime pine bark extract was associated with endothelial improvements in CVI (Fitzpatrick 1998) when 150 mg or 300 mg daily were compared with Daflon® at 1000 mg/day for eight weeks in a randomized trial (Cesarone 1996). Pycnogenol resulted in significant (p<0.05) improvements in rate of edema formation, resting ankle flux, and rate of ankle swelling, compared to Daflon treatment at both the lower dose and in the higher dose groups (Cesarone 2006). Limitations of these studies include lack of standardization of diagnostic criteria, and use of subjective scoring as opposed to standardized CEAP scoring (Martinez-Zapata 2008). The diagnostic methods for the comparison of blood flow in the extremities are also varied (Martinez-Zapata 2008). Comparatively, pycnogenol demonstrates higher improvements in endothelial CVI attributes (edema and its rate) compared with the more popular diosmin and hespiridin to date.
Obesity, Diet and Chronic Venous Insufficiency
A plenitude of research supports physical activity and weight management in the improvement of CVI (Brand 1988). Malonylodialdehyde (MDA), a by-product of lipid peroxidation created by oxidative stress was examined in a group diagnosed with 2nd or 3rd degree CVI (n=62) compared to controls. BMI was assessed as a covariable. Not surprisingly, MDA was higher in patients with cardiovascular disease compared with the control group (p < or = 0.0005), however, MDA concentration was also significantly higher in obese patients compared to those with a normal BMI (p < or = 0.001) (Kózka 2009). These findings bring further attention to the use of lifestyle and dietary modifications as a way to reduce markers of inflammation, impact NO concentration, and benefit CVI as well as CVD risk. Some nutritional agents that may also assist in this include: folic acid and its substrates, L-arginine, and non-genetically modified soy. L-arginine is an important substrate for NO production, while folic acid and its cofactors vitamin B6 and B12 reduce homocysteine levels that contribute to oxidative destruction of NO (Meletis 2006). Folate inhibits intracellular superoxide production, which increases the half-life of NO, allowing for greater vasodilation and further tissue protection (Meletis 2006). A diet emphasizing increased healthy fats, complex carbohydrates, and plant-based antioxidants as per the Mediterranean diet are beneficial in cardiovascular disease as well as CVI.
Future Directions for CVI: Influence of Estrogen
Women have a twofold higher incidence of CVI compared with men (Brand 1988). Serum levels of estradiol have been significantly associated with varicose veins, especially in post-menopausal women (Ciardullo 2000). Estrogen has been shown to upregulate vascular relaxation in the endothelium via nitric oxide (NO) and prostacyclin (PGI2) (Orsall 2004). Animal studies comparing the endothelium of male and female rats (n=12) have revealed significant sex differences in vasoconstriction/ relaxation, such as enhanced endothelium-dependent vasodilation and increased estrogen receptor activity in female rats, even independent of a NO pathway, suggesting there is an additional influence of estrogen on vasodilation, capable of acting synergistically with vasodilation effects of NO (Raffetto 2010). The influences of sex-hormone binding globulin (SHBG) and testosterone were also tested in the study, but were not found to influence varicose vein activity. Whether these findings can be replicated in human studies remains to be seen.
CVI is an early warning sign of cardiovascular disease. Reactive oxidative species are found in higher concentration in varicose tissues, and these respond well to interventions that reduce oxidative stress and enhance nitric oxide presence in kind, including acupuncture, horse chestnut seed extract, hespiridin and diosmin and an emphasis on healthy dietary habits. Comparing these interventions with compression therapy and better developing our understanding of the role of estrogen will lead to more effective treatment of CVI.
References
Abascal K and Yarnell E. Botanicals for Chronic Venous Insufficiency. Alt Complement Ther. 2007; 304-312.
Ahu ZX 1981. Research advances in the electrical specificity of meridians and acupuncture points. Am J Acup. 1981; 9:203-213.
Belcaro G. The role of transcutaneous PCO2 measurements in association with laser Doppler flowmetry in venous hypertension. Phlebology. 1988;3:189.
Belcaro G, Grigg M, Rulo A, Nicolaides AN. Blood flow in the perimalleolar skin in relation to posture in patients with venous hypertension. Ann Vasc Surg. 1989;1:5.
Bergan JJ, Schmid-Schonbein GW, Smith PD, Nicolaides AN, Boisseau MR, Eklof B. Chronic venous disease. N Engl J Med. 2006 Aug 3; 355(5): 488-96.
Brand FN, Dannenberg AL, Abbott RD, Kannel WB. The epidemiology of varicose veins: the Framingham Study. Am J Prev Med. 1988; 4(2): 96-101.
Braunwald E, Fauci AS, Kasper DL, Hauser SL, Longo DL, Jameson JL. Harrison’s Principles of Internal Medicine. 15th Edition. McGraw-Hill Professional, 2001. Burkitt DP. Some Diseases Characteristic of Modern Western Civilization; Occasional Review. British Medical Journal. 1973; 1: 274-278.
Carrasco OF, Ranero A, Hong E, Vidrio H. Endothelial function impairment in chronic venous insufficiency: effect of some cardiovascular protectant agents. Angiology. 2009; 60: 763-771.
Cassileth BR, Van Zee KJ, Chan Y, Coleton MI, Hudis CA, Cohen S, Lozada J, Vickers AJ. A safety and efficacy pilot study of acupuncture for the treatment of chronic lymphoedema. Acupunct Med. 2011;29:170–172.
Ciardullo AV, Panico S, Bellati C, Rubba P, Rinaldi S, Iannuzzi A, Cioffi V, Iannuzzo G, Berrino F. High endogenous estradiol is associated with increased venous distensibility and clinical evidence of varicose veins in menopausal women. J Vasc Surg. 2000 Sep; 32(3): 544-9.
Cesarone MR, Belcaro G, Rohdewald P, Pellegrini L, Ledda A, Vinciguerra G, Ricci A, Gizzi G, Ippolito E, Fano F, Dugall M, Acerbi G, Cacchio M, DiRenzo A, Hosoi M, Stuard S, and Corsi M. Comparison of Pycnogenol® and Daflon® in Treating Chronic Venous Insufficiency: A Prospective, Controlled Study. Clin Appl Thromb Hemost. 2006; 12: 205.
Danielsson G, Jungbeck C, Peterson K, and Norgren L. A Randomised Controlled Trial of Micronized Purified Flavonoid Fraction vs. Placebo in Patients with Chronic Venous Disease. Eur J Vasc Endovasc Surg. 2002; 23: 73-76.
Diehm C, Trampisch HJ, Lange S, Schmidt C. Comparison of leg compression stocking and oral horse-chestnut seed extract therapy in patients with chronic venous insufficiency. Lancet. 1996;347(8997):292-294.
Fitzpatrick DF, Bing B, Rohdewald P. Endothelium-dependent vascular effects of Pycnogenol. J Cardiovasc Pharmacol. 1998;32:509–515.
Halliwell B, and Gutteridge JMC. 2000. Free radicals in biology and medicine. 3rd edn. Oxford University Press.
Horse chestnut (Aesculus hippocastanum L.). http:// www.mayoclinic.com/health/ horse-chestnut/NS_ patient-horsechestnut [Accessed December 2 2011]
Georgescu A, Alexandru N, Popov D, Amuzescu M, Andrei E, Zamfir C, Maniu H, Badila A. Chronic venous insufficiency is associated with elevated level of circulating microparticles. J Thromb Haemost. 2009; 7: 1566–75.
Guzik TJ, Mussa S, Gastaldi D, et al. Mechanisms of increased vascular superoxide production in human diabetes mellitus: Role of NAD(P)H oxidase and endothelial nitric oxide synthase. Circulation. 2002; 105: 1656-1662.
Guzik B, Chwala M, Matuski P, Ludew D, Skiba D, Wilk G, Mrowiecki W, Batko B, Cencora A, Kapelak B, Sadowski J, Korbut R, Guzik TJ . Mechanisms of increased vascular superoxide production in human varicose veins. Archiwum Medycyny Wewnetrzej (Polish). 2011; 121 (9) 279-284.
Ignarro LJ. Biosynthesis and metabolism of endothelium-derived nitric oxide. Annu Rev Pharmacol Toxicol. 1990; 30:535–560.
Ignarro LJ, Fukuto JM, Griscavage JM, Rogers NE, Byrns RE. Oxidation of nitric oxide in aqueous solution to nitrite but not nitrate. Comparison with enzymatically formed nitric oxide from L-arginine. Proc Natl Acad Sci. 1993;90:8103–8107.
Kistner RL, Eklof B, and Masuda EM. Diagnosis of Chronic Venous Disease of the Lower Extremities: the “CEAP” Classification. Mayo Clin Proc. 1996; 71:338-345
Klaubunde, CM. Cardiovascular Physiology Concepts. Reactive Oxygen Species. Accessed April 2012 http://www.cvphysiology.com/Blood%20Flow/BF016.htm
Klaubunde CM. Cardiovascular Physiology Concepts. Nitric Oxide. Accessed April 2012. http://www.cvphysiology.com/Blood%20Flow/BF011.htm
Kózka M, Krzyściak W, Pietrzycka A, Stepniewski M. Obesity and its’ influence on reactive oxygen species (ROS) in the blood of patients with varicose veins of the lower limbs [Article in Polish]. Przegl Lek. 2009; (66): 213-7.
Krzyściak W and Kózka M. Generation of reactive oxygen species by a sufficient, insufficient and varicose vein wall. Acta Biochemica Polonica. 2011; 58(1): 89–94
Lewith GT, Field J, Machin D. Acupuncture compared with placebo in post-herpetic pain. Pain. 1983;17:361–8
Li S, Chen K, Wu Y, Jiao J, Tao L. Effects of warm needling at zusanli (ST 36) on NO and IL-2 levels in the middle-aged and old people. J Tradit Chin Med. 2003; 23:127-128.
Lorenz D, Marek ML. The active therapeutic principle of horse chestnut (Aesculus hippocastanum). Part 1. Classification of the active substance. Arzneimittelforschung. 1960;10:263-272. [Article in German]
Ma SX. Enhanced nitric oxide concentrations and expression of nitric oxide synthase in acupuncture points/meridians. J Altern Complement Med. 2003; 9:207-215.
Martinez-Zapata MJ, Bonfill Cosp X, Moreno RM, Vargas E, Capella D.
Phlebotonics for venous insufficiency (Review). The Cochrane Review 2008, Issue 4. Mears, Tim. Acupuncture for chronic venous ulcerations [Case report]. Acupuncture in Medicine. 2003; 21: 150-152.
McLafferty RB, Passman MA, Caprini JA, Rooke TW, Markwell SA, Lohr JM, Meissner MH, Eklöf BG, Wakefield TW, Dalsing MC. Increasing awareness about venous disease: The American Venous Forum expands the National Venous Screening Program. J Vasc Surg. 2008 Aug;48(2):394-9.
Meletis CD and Zabriskie N. Nitric Oxide, a Powerful Clinical Therapy. Alt Comp Therapies. 2006.
Mrwa U, Guth K, Haist C, et al. Calcium-requirement for activation of skinned vascular smooth muscle from spontaneously hypertensive (SHRSP) and normotensive control rats. Life Sci. 1986;38:191-196.
Orshal JM, Khalil RA. Gender, sex hormones, and vascular tone. Am J Physiol Regul Integr Comp Physiol. 2004;286:R233–R249.
Ottillinger B and Greeske K. Rational therapy of chronic venous insufficiency-chances and limits of the therapeutic use of horse-chesnut seeds extract. BMC Cardiovascular Disorders. 2001; 1:5.
Panigati D. The pharmacology of escin, a saponin from Aesculus hippocastanum L. II. Pharmacodynamics of escin. Chapter I. Boll Chim Farm. 1992;131:242-246. [Article in Italian]
Park JJ, Bang H. Methodological advances needed in analysis and interpretation of sham acupuncture validation studies. Acupunct Med. 2011 Sep; 29(3): 168-9.
Pittler MH and Ernst E. Horse chestnut seed extract for chronic venous insufficiency. Cochrane Database Systematic Review. 2004: (2): CD003230.
Pittler MH and Ernst E. Horse chestnut seed extract for chronic venous insufficiency. Cochrane Database Systematic Review. 2006 Jan 25;(1):CD003230.
Porter JM, Moneta GL. Reporting standards in venous disease: an update. International Consensus Committee on Chronic Venous Disease. Journal of Vascular Surgery. 1995; 21(4):635–45.
Raffetto JD, Khalil RA. Matrix metalloproteinases and their inhibitors in vascular remodeling and vascular disease. Biochem Pharmacol. 2008; 75: 346-359.
Raffetto JD, Qiao X, Beauregard KG, Khalil RA. Estrogen receptor-mediated enhancement of venous relaxation in female rat: implications in sex-related differences in varicose veins. J Vasc Surg. 2010 Apr; 51 (4): 972-81.
Robertson L, Evans C, Fowkes FG. Epidemiology of chronic venous disease. Phlebology. 2008; 23: 103-111.
Sirtori CR. Aescin: pharmacology, pharmacokinetics and therapeutic profile. Pharmacol Res. 2001;44:183-193.
Sprott H, Franke S, Kluge H, Hein G. Pain treatment of fibromyalgia by acupuncture. Rheumatol Int. 1998; 18(1): 35-6.
Takakura N, Takayama M, Kawase A, Yajima H. Double blinding with a new placebo needle: a validation study on participant blinding. Acupunct Med. 2011 Sep;29(3):203-7.
Tiffany, N et al. Horsechestnut: A multidisciplinary clinical review [from Natural Standard]. Journal of Herbal Pharmacotherapy. 2002; 2(1).
Tsuchiya M, Sato EF, Inoue M, Asada A. Acupuncture enhances generation of nitric oxide and increases local circulation. Anesth Analg. 2007;104:301-307.
Vas J, Modesto M, Mendez C, Perea-Milla E, Aguilar I, Carrasco-Lozano JM, Fasu V, and Martos F. Effectiveness of acupuncture, special dressings and simple, low-adhererence dressings for healing venous leg ulcers in primary healthcare: study protocol for a cluster-randomized open-labeled trial. BMC Complementary and Alternative Medicine. 2008; 8:29; 1472-6882.
Vein Clinics of America. Chronic venous insufficiency. http://www.veinclinics.com/ cme/skin-findings. html#ulcer. [Accessed December 9, 2011]
Yasim A, Kilinc M, Aral M, Oksuz H, Kabalci M, Eroglu E, Imrek. Serum concentration of procoagulant, endothelial and oxidative stress markers in early primary varicose veins.Phlebology/Venous Forum of the Royal Society of Medicine. 2008;23: 15–20.
Lovie Wesolowski-Spicer

Lifelong passion & purpose
With a passion for healing that began in adolescence, Lovie Wesolowski-Spicer has become an icon as health retailer and athletic performance coach.
By Carol Crenna • Photography by Mandy Harding
When the late Phil Brunner from Albi Naturals made a trip to the Prairies to introduce products to a new health retailer who’d contacted him, he arrived at the door of a teenager’s parents’ house. He was told the girl he wanted to meet wasn’t home from high school. He parked his Winnebago and tried not to look surprised as he waited for her, eyed closely by the cautious parents.
That was in 1977 when, at 17, Lovie Wesolowski-Spicer took daring steps to realize her dream to open a health store, cold-calling suppliers whose products she’d tried and trusted. With a $21,000 bank loan co-signed by her parents and another $7,000 from brother Jules, the enterprising youngster opened Nature’s Health Centre in Saskatoon’s Grosvenor Park Centre, a mall concept never attempted in Canada before. It opened under a business model and bookkeeping system that she developed in her grade 12 business class which she still uses today. Spicer has become a health and performance-nutrition pioneer, establishing the store in the same location for 35 years.
“I was fascinated by the human body at an early age, and asked for models or colouring books of the organs whenever I was offered a gift. Our family physician kept telling my parents about my affinity for healing, saying he conversed with me like a colleague when I was an adolescent,” states Spicer. Her strengths remain in chemistry – choosing product ingredients that are most effective, regardless of brand – and in building relationships with customers by giving health consultations.
At the same time she opened Nature’s Health Centre, Spicer became a sports nutrition coach, using her body-building brother as a guinea pig. She explains, “I felt, ‘If I can help people who are sick, can you imagine what I could do with people who are well?’” His lean body mass grew so large that athletes wanted to know his secret.
Spicer launched Performance Nutrition, a consulting company, and has worked with many famous athletes. She recounts notable names: Charles Servizio, in the Guinness Book of World Records for the most pushups (46,001 in 24 hours) was trained by her. Winnipeg Jets GM, Kevin Cheveldayoff has been a client since he played Juniors. Trainer-to-the-stars Grant Roberts, who trained Hilary Swank for Million Dollar Baby, was a customer at Spicer’s store when he was 15, and was then coached by her. Marcia Kilgore, owner of Bliss New York Spa, who has clients including Julia Roberts, worked for Spicer and continued getting advice while opening her business. Spicer advised Olympic bobsledder Jamie Cruikshank, Olympic decathloner Winchester Johnson, and Superbike racer Brett McCormick. She’s worked with NHL players Devin Setoguchi (Minnesota Wild) and Luke Schenn (Toronto Maple Leafs) since their teens. Agents asked Spicer to help increase the athletes’ muscle-to-fat ratio, enabling them to play in the NHL.
In 2004, former Saskatoon Blades GM Brent McEwen (current scout for Los Angeles Kings) asked Spicer to work with the team. She recounts, “The team had been dead last even though they had Mike Green, Wacey Rabbit and Devin Setoguchi, who later became some of the NHL’s highest paid players.” She created individual off-season programs for 33 on-ice players and 28 prospects. As a result, in one off-season, the average muscle gain per player was 22 pounds, and speed or endurance gains were extraordinary.
Now a Registered Nutritional Consultant (RNC), Certified Natural Health Practitioner (CNHP), and ISSA Specialist in Sports Nutrition, she lectures to national audiences.
Spicer has fond memories of working with health industry legends. Orthomolecular pioneer Dr. Abram Hoffer and Order of Canada recipient and pediatric expert Dr. John Gerrard visited her often because their patients shopped her store. She was taught by icons Dr. Morton Walker, Dr. Bernard Jensen and Dr. Earl Mendell. She knew Udo Erasmus as a zoologist before he launched his product line and lectured at her store, and the late Charlie Fox, Kyolic’s founder, was “a phenomenal storyteller” during his store lectures.
Jack Gahler, a construction worker who sold supplements part-time, didn’t have initial success with Spicer. “I didn’t like the products he sold, so wouldn’t buy them, and encouraged him to start a higher-end line. He did, and called it Natural Factors. Jack’s fibre is woven into the structure of the industry; grandson Michael stays true to his grandfather’s humbleness and integrity.”
Spicer obtained a second business loan a decade ago when health products went mainstream –– her biggest-selling brand was introduced in the mall’s supermarket. “I invested in introducing products that no other store had to regenerate the lost business. It worked.”
Today, in her 50s, Spicer continues coaching and managing the store every day and now greets third-generation customers. How does she keep going, even after raising eighteen-year-old twins? She concludes, “There was never any choice. I was brought to where I need to be. I still feel 17, having the same passion, and living by the same philosophies.” Spicer has now committed to writing a book to “give back” to the hockey industry.
Spicer’s sage advice:
• Hire up-and-coming experts. Spicer heads to the local university to find staff. Four staff members became naturopathic physicians during their employment. Biochemistry student, Jason Kindrachuk, worked at the store for years, and is now a Ph.D. researcher at National Institute of Allergy and Infectious Disease, Washington D.C.
• Create environments to keep staff. She has never fired an employee and no one has left for reasons other than to advance their medical careers. (Some felt the responsibility to find a replacement when they left.) Their needs and limited hours available are respected; they’re given unique opportunities to learn; they’re treated like family Beckie Harris has been there for 22 years.
• Align with health organizations. Patient-support organizations are realizing that research-backed dietary advice brings increased hope to those with a disease. It empowers them to participate in their healing. “Providing a local health society with specific nutrition and supplements that relieve symptoms offers huge potential for a store (or supplier) to get in on the ground floor.” While on the provincial board of the MS Society, Spicer became the consulting expert, fielding all complementary medicine and nutritional questions.
• Consider public profile. People of influence can become champions of your company. Public speakers in all sectors, who have incredible opportunities to influence audiences, often mention nutrition. “At a teachers’ conference, in the middle of the keynote speaker’s lecture to 2,500 people, he stopped and said, ‘I have to share with all of you that you need to be taking omega-3s for these reasons… I take Ascenta.’” Immediately following, attendees purchased every bottle in Spicer’s store.
• Don’t dismiss any request. Seemingly unrelated sectors provide potential customers. Spicer has conducted health talks for a musicians’ association about stress reduction; a mining company’s miners about detoxification and sinus-cavity cleansing; and a violin players’ organization discussing relief for muscle pain due to holding instruments for long periods.
• Stay ahead of the curve to be seen as a leader, but not too far ahead. When the first omega-3 supplier tried to sell the new product to Spicer, she repeatedly refused. Spicer waited and watched the market. After the first reports by media validating its research, and disease-management organizations beginning to promote it – areas outside of the natural health industry Spicer suddenly placed a large order. “Surprised, they called and asked why the sudden change of mind. I said ‘because the environment changed.’ It must be fresh when the trend hits the marketplace.”
• Be a trend forecaster. Spicer analyzes cultural trends, searches websites like www.webmed.org for new compounds being researched, and keeps an eye on new specialty retailers for the latest trends. “Take an ‘aerial’ view of nutrition that’s now a part of everyday everywhere school, restaurants, fitness, workplace wellness, retirement homes, vacation destinations…” Her picks for future trends:
1. Tea will top sales. Since tea shops/public tea rooms are growing, increasing tea consumption, this will translate into a lucrative healthy tea product market.
2. Yogurt makes resurgence. Frozen yogurt shops are returning; and similar to how juice bars inspired sales of greens and protein powder, superfood ingredients added to yogurt will spur supplement sales to “make your own.”
3. Weight loss will expand. “Diet products provide an opportunity for you to become consultants on the other necessary steps that should be taken for weight management when customers come into the store.”
• Think collaboration, not competition. Spicer aligned herself with the departments of pharmacy and medicine at the University of Saskatchewan, and advises medical students there on complementary medicine. “Open communication has created mutual respect. If you consider that all disciplines are trying to help in their own way, no one gets defensive and everyone works together.”
• Recognize regulatory cycles. Spicer explains, “Ever since I began, there have been government regulation issues and products pulled from shelves. It doesn’t have to impact the business.” Within first years of business, fears from the U.S. that all supplements would be pulled from the market prompted her to include product availability-dependent back-out clauses in her leases. She advises not concentrating the business in one area, and focusing less on product hype and more on core customer needs.
At a Glance
Nature’s Health Centre
Locations: One
Main Address: 48 Grosvenor Park Shopping Centre, Saskatoon
Phone: (306) 373-5322
Website: www.natureshealthcentre.com
Staff: 4
Top-Selling Products
Food: essential fats and oils, gluten-free alternative grains, gluten-free mixes (cookies, muffins, brownies)
Vitamins: foundation vitamins and minerals including vitamin C, vitamin B, magnesium, calcium, weight management products, athlete-focused products including sports nutrition and protein powders
Personal: Fragrance-free, preservative-free, hypoallergenic shampoos, conditioners and skin ointments for specific health issues
$27B tobacco lawsuit headed for Quebec court
Canada’s three main tobacco companies are battling in a Montreal court in the biggest civil case in Canadian history. A group of Quebec smokers is suing Imperial Tobacco Canada, Rothmans, Benson & Hedges, and JTI-Macdonald, claiming the companies failed to properly warn customers about the dangers of smoking, underestimated evidence relating to the harmful effects of tobacco, engaged in unscrupulous marketing, and destroyed documents. It is the first time tobacco companies have gone to trial in a civil suit in Canada and up to $27 billion in damages and penalties are at stake. Six provinces are also teaming up to sue Canadian tobacco firms for health-care costs; British Columbia, New Brunswick, Nova Scotia, Saskatchewan, Manitoba, and Prince Edward Island are retaining a national legal team to help them prosecute Canadian tobacco companies in an effort to recover billions of dollars.
Study debunks ionic footbath detox claims
Researchers from the Canadian College of Naturopathic Medicine (CCNM) and the University of Toronto’s Faculty of Pharmacy conducted a series of tests running an ionic footbath with and without feet and analyzed the water for differences in the level of potentially toxic elements (PTEs). The water was first measured after running the machine without feet using both distilled and tap water. Weekly measurements were then conducted on six healthy participants who used the machine with tap water once a week for four weeks. No differences were found in toxic metals that were leached into the water whether or not feet were in the water, including lead, cadmium, and arsenic. On the other hand, a significant increase in some of the same elements present in the metal array used in the footbath to generate an electric current in the water was found. Over time, the array corroded and elements from this corrosion caused the water to become dirty and cloudy and change color. The study also failed to find any evidence to suggest that the machine increased the body’s ability to excrete the heavy metals. J Environ Public Health. 2012;2012:258968. PMID: 22174728





