





Dr. Louis Hugo Francescutti was installed as president of the Canadian Medical Association (CMA) during the association’s 146th annual meeting in Calgary. Dr. Francescutti succeeds Dr. Anna Reid, an emergency physician at Stanton Territorial Hospital in Yellowknife. “I feel strongly that Canada’s doctors can come together to transform our health care system into a system that will better serve our patients,” said Dr. Francescutti. “The evolving needs of Canada’s rapidly aging population mean there is no better time for the profession to shine.” Born in Montréal, Dr. Francescutti received his combined Doctor of Philosophy (Immunology) in 1985 and his Doctor of Medicine in 1987 from the University of Alberta.
In 1994, he completed further studies in injury control while working toward a Masters of Public Health at Johns Hopkins University in Baltimore, Maryland. Dr. Francescutti currently works as an emergency physician at the Royal Alexandra Hospital and the Northeast Community Health Centre in Edmonton. As a professor in the School of Public Health at the University of Alberta, Dr. Francescutti has taught courses in injury control, public health and advocacy. Dr. Francescutti will serve as president of the CMA until August 2014.
Dr. Louis Hugo Francescutti New President of the Canadian Medical Association
Phase III Study of Investigational Vaccine in Canada to Prevent Clostridium difficile
Sanofi Pasteur, the vaccines division of Sanofi announced the initiation of its Phase III clinical program called Cdiffense to evaluate the safety, immunogenicity and efficacy of an investigational vaccine for the prevention of primary symptomatic Clostridium difficile infection (CDI). Clostridium difficile (C. diff) is a potentially life-threatening, spore-forming bacterium that causes intestinal disease. The risk of C. diff increases with age, antibiotic treatment and time spent in hospitals or nursing homes, where multiple cases can lead to outbreaks. The investigational C. diff vaccine is designed to produce an immune response that targets the toxins generated by C. diff bacteria, which can cause inflammation of the gut and lead to diarrhea. The investigational vaccine stimulates a person’s immune system to fight C. diff toxins upon exposure and ultimately may help prevent a future infection from occurring. The Cdiffense Phase III clinical program has just started recruiting volunteers in Canada for a randomized, observer-blind, placebo-controlled, multi-center, multi-national trial that will include up to 15,000 adults at 200 sites across 17 countries. Volunteers for the study should be age 50 or older and planning an upcoming hospitalization or have had at least two hospital stays and have received systemic antibiotics in the past year. For more information on the Cdiffense trial, please visit www.Cdiffense.org.
GeneDx Introduces Advanced Genetic Test Panels for Breast and Colon Cancer
GeneDx, one of the world’s foremost genetic testing laboratories and a wholly-owned subsidiary of Bio-Reference Laboratories, Inc. has announced the launch of a comprehensive suite of genetic tests for inherited cancer, including a 26-gene panel for breast and ovarian cancer that includes BRCA1 and BRCA2 and next generation sequencing based multi-gene panels for colorectal cancer, pancreatic cancer, and endometrial cancer. GeneDx, the first commercial laboratory to utilize next generation sequencing technologies in a CLIA-environment, is among only a handful of commercial labs currently offering testing for inherited cancer. The laboratory will begin accepting specimens immediately. The test offerings include a rapid turn-around test of the BRCA1 and BRCA2 genes combining sequencing and deletion/duplication analysis; an Ashkenazi Jewish panel for the three common Ashkenazi Jewish founder mutations in BRCA1 and BRCA2; a 26-gene panel for breast and ovarian cancer; an 18-gene panel for pancreatic cancer; an 18-gene panel for colorectal cancer; and an 11-gene panel for endometrial cancer. The test panels, which are marketed as OncoGeneDx, also include a Comprehensive Cancer Panel of 35 genes. All panels include deletion/duplication assessment.
Effects of habitual coffee consumption on cardiovascular health and all-cause mortality

The biological effects of coffee may be substantial and are not limited to the actions of caffeine. Coffee is a complex beverage containing hundreds of biologically-active compounds and the health effects of chronic coffee are wide-ranging. This review examined the effects of coffee consumption on cardiovascular health and all-cause mortality. From a cardiovascular standpoint, coffee consumption may reduce the risks of type 2 diabetes mellitus and hypertension, as well as other conditions such as obesity and depression, but it may adversely affect lipid profiles depending on how the beverage is prepared. A growing body of data suggests that habitual coffee consumption is neutral to beneficial regarding the risks for a variety of adverse cardiovascular outcomes, including coronary heart disease, congestive heart failure, arrhythmias, and stroke. Large epidemiological studies suggest that regular coffee drinkers have reduced risks for mortality, both cardiovascular and all-cause. The potential benefits also include protection against neurodegenerative diseases, improved asthma control, and lower risk of select gastrointestinal diseases. Most of the data are based on observational data, with very few randomized controlled studies and an association does not prove causation. J Am Coll Cardiol. 2013 July. PMID: 23871889
Exercise to improve sleep in insomnia: bidirectional effects

Exercise improves sleep quality, mood, and quality of life among older adults with insomnia. This study evaluated the daily bidirectional relationships between exercise and sleep in a sample of women with insomnia. Participants included 11 women with insomnia who engaged in 30 minutes of aerobic exercise 3 times per week. Self-reported sleep quality was assessed at baseline and at 16 weeks. Sleep and exercise logs and wrist activity were collected continuously. The results showed that total sleep time, sleep efficiency, and self-reported global sleep quality improved from baseline to 16 weeks. Baseline ratings of sleepiness were negatively correlated with exercise session duration. Daily exercise was not associated with subjective or objective sleep variables during the corresponding night. However, participants had shorter exercise duration following nights with longer sleep onset latency. Total sleep time at baseline moderated the daily relationship between total sleep time and next day exercise duration. The relationship between shorter total sleep time and shorter next day exercise was stronger in participants who had shorter total sleep time at baseline. The authors conclude sleep influences next day exercise rather than exercise influencing sleep and that improving sleep encourages exercise participation. J Clin Sleep Med. 2013 August. PMID: 23946713
Low CSF concentration of mitochondrial DNA in preclinical Alzheimer’s disease

This study attempted to identify a novel biochemical marker that precedes clinical symptoms of Alzheimer’s disease (AD). Using quantitative PCR techniques, the authors measured circulating cell free mitochondrial DNA (mtDNA) in cerebrospinal fluid (CSF) from study participants, selected from a cohort of 282 subjects that were classified according to their concentrations of Aβ1-42, t-tau and p-tau and by the presence or absence of dementia, including asymptomatic subjects at risk of AD, symptomatic patients diagnosed with sporadic AD, pre-symptomatic subjects carrying pathogenic PSEN1 mutations and patients diagnoses with Fronto-temporal Lobar Degeneration (FTLD). They performed equivalent studies in a separate validation cohort of sporadic AD and FTLD patients. They easured mtDNA copy number in cultured cortical neurons from mutant Amyloid Precursor Protein/Presenilin1 transgenic mice. The results showed that asymptomatic patients at risk of AD and symptomatic AD patients, but not FTLD patients, exhibit a significant decrease in circulating cell free mtDNA in the CSF. The authors conclude that the low content of mtDNA in CSF may be a novel biomarker for the early detection of preclinical AD. These findings also support the hypothesis that mtDNA depletion is a characteristic pathophysiological factor of neurodegeneration in AD. Ann Neurol. 2013 Jun. PMID: 23794434
Francesco Anello, MD

Excellence in Integrative Medicine
The path taken by Dr Francesco Anello to arrive at the creation of the Complementary Healing Arts clinic in Cambridge, Ontario is indeed unique and influenced by several phenomena outside of any one individual’s control. Yet the story unfolds in a manner familiar to IHP readers: rigorous training in conventional therapeutics, considerable time spent applying the conventional medical model, a feeling of being “unfulfilled” by the care being delivered, and the inevitable search for better solutions to common, debilitating problems.
Francesco Anello, MD
Dr Anello completed his undergraduate (HBSc genetics) and medical training at the University of Western, completing a family practice residency in 1984. He opened a family practice in Cambridge in 1986, providing a full- spectrum of care, yet with emphasis on obstetrics and neonatal/ pediatric care, and maintained emergency room rotations and surgical assisting at a local hospital. The healthcare crisis of the mid 1990’s and accompanying cutbacks left Dr Anello feeling the style of practice he was engaged in was no longer tenable. He closed down his private practice and undertook a role with the Woolwich Community Health Centre in 1995. At the same time, he began building what is known today as the Complementary Healing Arts clinic, which he fully transitioned to in 2002.


Dr Anello always maintained an active interest in integrative medicine. His original conventionally- focused facility in 1986 was seeing a lot of obstetrics patients, and quickly his clinic gained a reputation as being “midwife friendly”. In Dr Anello’s words, “a holistic perspective on birthing was required… people were wanting it, asking for it”. His work during a locum in the town of St Jacobs served as an excellent introduction to more holistic birthing practices, as he served a large Mennonite community within the town. The roots of Dr Anello’s interest in integrative medicine began much earlier, however. During his last year of medical school, Francesco spent six months in India completing a rotation in obstetrics and infectious disease. He met up with an individual he described as a “wandering healer” whom he spent the majority of the trip with, and was introduced to the art of meditation. Shortly after his return to Canada, Dr Anello continued his pursuit of training in integrative medicine through a channel familiar to most integrative MD’s; the seminars hosted by Jeffrey Bland and Alan Gaby.
The clinic is situated in a stunning, large home on a main street in Cambridge, Ontario. An initial visit with Dr Anello is a one- hour intake, involving a complete medical history, a battery of common lab tests, and discussion of one or two relevant integrative diagnostic tests. Subsequent visits review relevant laboratory outcomes, an individualized treatment plan specific to the patient is created, and Dr Anello plus the impressive support staff of the facility implement recommendations as a team. The clinic performs a large number of IV therapies, used to address a wide array of patient concerns. Chief among them is the reputation the clinic has garnered as a facility of cardiovascular disease management, with IV EDTA emerging as among the most relied upon interventions.
The team at the Complementary Healing Arts clinic is as diverse and skilled as the clinic’s founder. Marianne Anello brings a wealth of clinical experience as an RN in a broad array of hospital settings including ER and pediatric nursing. At the facility Marianne oversees laboratory testing and IV therapies. Michael Reid is an ND graduated from CCNM. He describes Dr Anello as a gifted, selfless, and extremely knowledgeable practitioner of integrative medicine, citing his time with Dr. Anello as helping him advance his skill set as an ND. Alex Audette is an Asian- trained physician of traditional Chinese medicine. (broadskypartners.com) In addition to conventional TCM practices, Dr Audette delivers Japanese deep tissue lymphatic drainage at the facility, a labour- intensive, hands on form of acupuncture that may be time consuming yet delivers important outcomes quickly for patients. The clinic also boasts highly skilled and experienced practitioners in psychotherapy (Kristin Trotter, PhD), and registered nurse (Donna Rieck). Trudy Schneider rounds out the team by acting as office manager.
Dr Anello did not let me spend much time getting to know about his style of practice. Instead, he would make a comment about some new happening in the world of medicine, and I would eagerly delve into the topic mostly out of personal interest. It began with a discussion of Dr Garth Nicolson, formerly Professor and Chairman of the Department of Tumor Biology at the University of Texas M.D. Anderson Cancer Center, who investigated the cause of Gulf War Syndrome with all the tools of molecular biology he had at his disposal. He hypothesized a mycoplasma organism was weaponized and used against US soldiers. The organism is believed to be responsible for chronic fatigue, chronic rheumatic pain type syndromes common among soldiers who served in the gulf war. Dr Nicolson has developed a private lab that tests for the mycoplasma organism, and advocates for the use of intermittent doxycycline for treatment of the disorder. Most astonishing to me, a handful of days before my interview with Dr Anello, a surgeon from the US was claiming 50%+ of individuals seeking back surgery for chronic pain can avoid the surgery entirely with an aggressive six month course of antibiotics.


I asked Dr Anello about the CPSO, and whether or not he has faced controversy from them. He described a few inquiries, all of which occurred in his first 10 years of practice. I was then immersed in a fascinating discussion of a well- known Ontario physician, Jozef Krop. Dr Krop practiced integrative medicine in Ontario for many years, and was cited as a major contributor to the modern integrative practices that define management of chemically sensitive patients. Dr Krop found himself in a lot of trouble with the CPSO, yet his patients rallied at Queen’s Park and not only vindicated Dr Krop, but also helped to pass the Kwinter Bill in Ontario. In brief, the Bill enshrined a patient’s freedom of choice in healthcare, and went a long way in preventing the stripping of a medical license for reasonable practice outside of conventional scope for physicians in Ontario.

IHP is grateful to Dr Anello and the Complementary Healing Arts team for allowing us to showcase their efforts to you. Dr Anello embodies everything one hopes to encounter in a practitioner of integrative medicine, and like a handful of others we have had the privilege to meet, he arrived at his current destination during a time when the path was much more difficult to follow than it is today. I am normally quite good at keeping an interview with integrative MD’s focused on the type of information gathered for a story. Dr Anello’s passion and knowledge simply made the task impossible in this case. Every side- bar, story, “hey did you hear this?” had me mesmerized and fascinated. Francesco truly is a wealth of knowledge and wisdom… Our profession will be richly rewarded if we can pry him from his clinic and get him delivering a lecture circuit of his own? Dr Anello, you are likely to serve as the “wandering healer” who inspires the next generation of physician to deliver the best system of medicine going…
Cognitive health and new technologies

Cognitive health and new technologies
Are you ready to prescribe videogames?
Abstract
In the face of a growing incidence of cognitive decline there is a need for sustainable lifestyle interventions to support, maintain and improve cognitive health. Perhaps serendipitously or intentionally technological evolution delivers a novel medium for cognitive training filled with promise and new potential. This medium is the realm of virtual reality, video games and mobile devices that allow for the development of individualized training regimes tailor made to suit the patients’ needs, not to mention a virtual intelligence that may be able to preserve that which the brain can no longer contain. This review explores the research behind the application of video games to cognitive exercise, rehabilitation programs encompassing virtual realities and smart phones dedicated to maintaining access to faculties challenged by the progression of Alzheimer’s disease. The limitations and challenges of these interventions will be explored as well.
Introduction
As the baby boomers continue to age, the incidence of mild cognitive decline, as well as Alzheimer’s disease (AD) and dementia, is expected to rise (Park 2003). Currently the prevalence of Alzheimer’s disease is 1% in persons 60-70 years of age and 6-8% in those over 85 (Mayeux 2010), while the prevalence of mild cognitive impairment is 10-20% in the 65 and older population (Petersen 2011). There is a growing need for lifestyle interventions that are effective, economically sustainable and compliance-friendly.
Some of the early signs of cognitive decline can include mild memory loss, mild reduction in reasoning, processing speed, and executive function, such as attention, language, and visuospatial skills (Deary 2009, Petersen 2011). These may be a result of normal aging (age-associated cognitive decline), mild cognitive impairment (slightly more significant cognitive decline than that of normal aging) as well as more serious causes such as Alzheimer’s disease, hypothyroidism, vitamin B12 deficiency, cerebrovascular disease (i.e. vascular dementia), central nervous system infection, hydrocephalus, cancer, substance abuse, adverse effects of medications, HIV related cognitive disorder and others (Mayeux 2010). A reduction in verbal memory and executive function, coupled with reduced retention of newly acquired information are more indicative of Alzheimer’s disease, while memory loss associated with psychosis is more characteristic of dementias (Mayeux 2010).
A reduction in verbal memory and executive function, coupled with reduced retention of newly acquired information are more indicative of Alzheimer’s disease, while memory loss associated with psychosis is more characteristic of dementias (Mayeux 2010). As computers and mobile devices become more mainstream, their application to cognitive health may offer a novel intervention that is inexpensive and customizable, able to address individual needs of patients. Evidence from a recent prospective study correlates the use of daily computers with 30-40% lower risk of dementia (Almeida 2012). Healthy men, 5506 participants 69-87 years of age, were followed for six years, with the primary outcome documented being the diagnosis with dementia. Computer use included browsing the internet, e-mail, word processing and playing games. Though there may be a range in the degree of benefit from computer use, potentially dependent on quality of content viewed, one simple factor that does seem to have an effect is experience. Comparing the functional MRI recordings of experienced users with those not familiar with the internet, Small et al (2009) found that the regular use correlated with activation of brain areas associated with decision making and complex reasoning, while naive internet browsing resulted in activation of areas associated with reading only. Thus there is some evidence to support the use of computers in the elderly population as a means to promote cognitive health. This review will examine a few computer based interventions and their impact on cognitive function as well as their respective limitations.
Video Games
A systematic review by Kueider et al (2012) provides an excellent overview of the terrain of video games and their current potential. Eight studies (participants ages 50-87) were examined and their impact on cognition compiled. Some of the games included were Nintendo Wii’s Big Brain Academy, Rise of Nations, Medal of Honor, Pac Man, Donkey Kong, Tetris, Atari: Break out, Crystal Castles, Galazian, Frogger, and Kaboom. These were played between two to 11 weeks for two to five hours each week. The biggest improvements were made in reaction time (effect size of 0.77; in this case the closer the effect size is to 1.0 the stronger the effect), processing speed (0.72) and global cognition (0.69). Global cognition was evaluated using the WAIS-R full IQ and ADAS-Cognition. A milder impact was made on executive function (0.25) and attention (0.21). The degree of impact varied across the different games examined. Except for Brain Academy, none of the above mentioned games focus on improving cognitive function.

Contradictory to popular belief games stereotypically seen as “intellectual” do not necessarily yield cognitive improvements, as demonstrated by study by Boot et al (2013). Healthy participants (mean age 74yo) randomized to play 60 hours of Brain Age 2 (intellectual game) or Mario Kart (action game) were assessed using a battery of cognitive tests including flanker test (selective attention), meaningful memory, Raven’s matrices (reasoning), visual search (processing speed) and others. No significant changes were reported after 12 weeks for either game.
To determine which game type offers the most cognitive benefit Oei et al (2013) compared several different types of games in the undergraduate student population. Seventyfive participants were randomly assigned to one of the five games: memory matrix (reproduce a sequence), The Sims (life simulation), action (first person shooter), match-3 (Bejewelled 2), or hidden-object (find object within a complex visual scene). They were instructed to play for one hour/day, five days per week for four weeks (20 hours total). They were assessed using a wide array of cognitive tests pre and post the games intervention. The tests included attentional blink, filter task, visual search/spatial memory and complex span. The action game resulted significant improvement in attentional blink (p<0.001). Authors speculate this to be due to the need to rapidly switch attention between targets, specific to the nature of action games, which results in improved attention switching transferrable to tasks outside the game. The action game also resulted in improvements in filter task, the ability to track multiple objects simultaneously, and complex span, a combination of arithmetic and verbal memory tasks, while Bejewelled-2 yielded positive results on visual search/ spatial memory and complex span. Memory matrix and hidden-object were beneficial for visual search/spatial memory only, while the Sims did not make a significant impact on any of the four parameters. Thus it would seem that the action game offers to most broad benefit, though some cognitive benefit can be extracted from the other games as well.
Virtual Training
Though potentially less entertaining than video games, virtual reality (VR) training programs designed to improve specific skills are delivering effective interventions to both healthy elderly participants and those suffering with Alzheimer’s disease. A study by Optale et al (2010) demonstrated positive effect of VR training on several cognitive parameters in healthy elderly population. The randomized control trial enrolled 36 participants (mean age 80yo) with various degrees of impairment on the Verbal Story Recall (VSR) test into control (music therapy) and experimental groups. The experimental group received three training sessions every two weeks consisting of auditory training; listening to an audio recording of three different stories with three different musical backgrounds, and VR training; finding the correct path to a viewing location of a 15 second film clip, using a joystick and computer while listening to the same background music as used in the audio training. The training was delivered for three months. The training resulted in significant improvements in Mini Mental State Examination (MMSE) (p=0.014), Digit Span test (short term verbal memory; p=0.043), VSR (p<0.001), Phoenemic Verbal Fluency (p=0.005), Geriatric Depression Scale (p=0.025), while the control group either maintained or demonstrated loss of function. No changes were observed in visuospatial processing and activities of daily living.
Using VR as a safe and controlled training environment, Hofmann et al (2003) created a shopping intervention to improve daily living function of patients with AD. The VR experience was created using digital photographs of the shopping route, which the participants were required to navigate in order to locate the shop, buy three items and answer 10 relevant multiple choice questions, such as “you will have to cross this road to get to the pharmacist. What do you have to keep in mind?”. After 12 sessions over four weeks, a significant reduction in the number of mistakes made (p<0.044) was documented, which was sustained for three weeks following the training. No impact on the MMSE was observed. While the study demonstrated ability to improve specific skills, it is difficult to conclude how generalizable these gains are to real-life shopping experience, as well as the duration of their perseverance past the three week follow up.
Other ways of applying new technologies
As the world of games and virtual realities continues to evolve, so does the world of applications. A case study by De Leo et al (2011) capitalized on the photographical capacity of the smart phone and developed what could be termed as virtual memory for a patient with Alzheimer’s disease. The participant was diagnosed with stage 4 Alzheimer’s disease (according to Functional Assessment Staging (FAST)) and was given a programmed smart phone, which he wore around his neck for four weeks. The phone was programmed to capture pictures every five minutes between 8:00am and 8:00pm. The images were uploaded automatically to a server at 2am each night. Redundant and poor quality images were discarded by the research team, and the rest were made into a slideshow, which the participant viewed once a week. A recent events memory recall test was administered before and immediately after viewing the video, along with a five-point Likert scale satisfaction questionnaire. Not surprisingly there were more events remembered with the slideshow than without. Though the participant did not agree that the slideshow was a very useful tool as memory aid, he did agree that it made him feel less anxious knowing that it was keeping a record, especially in social situations where he was concerned about forgetting who he has met. Being able to share the experiences with family through the slideshow was an added pleasure. The device did not pose an inconvenience to the participant but did present with some technological problems and dependency on a video editor to sort through the slideshow.
Another approach to creating a virtual memory is currently in the process of being piloted. Donnelly et al (2008) developed a Cell-Phone-Based-Video Streaming System to provide routinely scheduled reminders to patients with dementia as a way to assist with daily activities. By using familiar faces of relatives, the authors hope to achieve higher compliance. Another potential application of the smart phone is the use of the GPS component as way of locating patients with Alzheimer’s disease that become lost (De Leo 2011). The application of the Wii is another area that can be explored, as well as the social benefit and cognitive impact of the virtual online communities, such as Facebook, online dating and Skype.

Challenges and Limitations
There were two main obstacles identified in the literature with respect to these new technologies. The first and most familiar is the challenge of compliance. Boot et al (2013) explored participant preferences in a study comparing two different Nintendo DS game interventions. Participants (mean age 74yo) were randomized to play 60 hours of either an action game, Mario Kart DS, or a more intellectual game, Brain Age 2, which included choice of several different games including Sudoku. Participants rated the intellectual game more enjoyable and were more compliant with the prescription (56 hours on average were played of Brain Age 2 compared to 22 hours of the Mario Kart). They described the Mario Kart as “mindless” and “utterly boring”. Ironically, according to the research (Boot 2013, Oei 2013), it is the action games that offer the most benefit with respect to executive function and reaction speeds. The other concern is the adverse events associated with the ergonomics of computers. Some of the reported side effects of desktop monitors, joysticks and keyboard use included eye strain and arthritis (Boot 2013), while use of head-mounted visual displays, typically used to create virtual realities, resulted in nausea, vomiting, dizziness, headaches, disorientation and transient vestibular and psychomotor disturbances (Cherniak 2011). Another complication though not discussed in detail in the literature, but very familiar to us all, is the frustration of technological limitations in the forms of hardware and software malfunctions. Despite these challenges, a systematic review by Kueider et al (2012) reports that participants do not need to be technologically savvy in order to enjoy all the benefits that these intervention have to offer with respect to cognitive health.
Conclusion
As the technological world continues to evolve it may offer new tools and approaches that may aide in the maintenance of cognitive health and in the rehabilitation of various cognitive impairments. Individual needs and preferences will become crucial in the development of efficacious video games and virtual realities, which will not only need to stimulate the cognitive functioning but maintain interest and intrigue the participant, ideally while connecting them to a strong and supportive social network.
References:
Almeida OP, Yeap BB, Alfonso H, Hankey GJ, Flicker L, Norman PE. Older men who use computers have lower risk of dementia. PLoS One. 7(8) (2012)
Basak C, Boot WR, Voss MW, Kramer AF. Can training in a realtime strategy video game attenuate cognitive decline in older adults? Psychology of Aging. 23(4) (2008); 765-77
Boot WR, Champion M, Blakely DP, Wright T, Souders DJ, Charness N. Video games as a means to reduce age-related cognitive decline: attitudes, compliance, and effectiveness. Front Psychology. 4(31) (2013)
Cherniack EP. Not just fun and games: applications of virtual reality in the identification and rehabilitation of cognitive disorders of the elderly. Disabil Rehabil Assist Technology. 6(4) (2011); 283-9
Cohen GD, Firth KM, Biddle S, Lloyd Lewis MJ, Simmens S. The first therapeutic game specifically designed and evaluated for Alzheimer’s disease. Am J Alzheimer’s Dis Other Demen. 23(6) (2008): 540-51
De Leo G, Brivio E, Sautter SW. Supporting autobiographical memory in patients with Alzheimer’s disease using smart phones. Applied Neuropsychology. 18(1) (2011); 69-76
Deary IJ, Corley J, Gow AJ, Harris SE, Houlihan LM, Marioni RE, Penke L, Rafnsson SB, Starr JM. Age-associated cognitive decline. Br Med Bull. 92 (2009); 135-52
Donnelly MP, Nugent CD, Craig D, Passmore P, Mulvenna M. Development of a cell phone based video streaming system for persons with early stage Alzheimer’s disease. Conf Proc IEEE Eng Med Biol Soc. 2008; 5330-3
Hofmann M, Rosler A, Schwarz W, Muller-Spahn F, Krauchi K, Hock C, Seifritz E. Interactive computer-training as a therapeutic tool in Alzheimer’s disease. Compr Psychiatry. 44(3) (2003): 213-9
Kueider AM, Parisi JM, Gross AL, Rebok GW. Computerized cognitive training with older adults: a systematic review. PLoS One. 7(7) (2012)
Mayeux R. Clinical practice. Early Alzheimer’s disease. New England Journal of Medicine. 362(23) (2010): 2194-201
Oei AC, Patterson MD. Enhancing cognition with video games: a multiple game training study. PLoS One. 8(3) (2013)
Optale G, Urgesi C, Busato V, Marin S, Piron L, Priftis K, Gamberini L, Capodieci S, Bordin A. Controlling memory impairment in elderly adults using virtual reality memory training: a randomized controlled pilot study. Neurorehabilitation Neural Repair. 24(4) (2010); 348-57
Park HL, O’Connell JE, Thomson RG. A systematic review of cognitive decline in the general elderly population. Int J Geriatric Psychiatry. 18(12) (2003): 1121-34
Petersen RC. Clinical Practice. Mild Cognitive Impairment. New England Journal of Medicine. 364(23) (2011): 2227-34
Small GW, Moody TD, Siddarth P, Bookheimer SY. Your brain on Google: patterns of cerebral activation during internet searching. Am J Geriatr Psychiatry. 17(2) (2009); 116-26
Hydrotherapy

Hydrotherapy
Evidence For Clinical Applications
Abstract
Hydrotherapy is the use of water for therapeutic purposes. The mechanisms of action of hydrotherapy include local vasoconstriction followed by reflexive vasodilation which activates cutaneous circulation. The resulting therapeutic actions include muscle relaxation, enhanced collagen flexibility, pain reduction, and anti-inflammatory effects. Many acute and chronic health conditions can benefit from these effects. The limited evidence available for the most common uses of hydrotherapy is reviewed. Hydrotherapy is effective for both rheumatoid arthritis and osteoarthritis, providing reductions in pain, increased mobility, and improved quality of life. The evidence shows that hydrotherapy is not effective in reducing the incidence, duration, or severity of the common cold in children. For patients suffering from chronic heart failure, hydrotherapy improves exercise tolerance and the hemodynamic profiles of patients, including beneficial reductions in blood pressure and heart rate. Considered together, the existing studies suggest that hydrotherapy is an extremely safe treatment option for a variety of health conditions.
Introduction
In general, hydrotherapy is the use of hot and cold water for the maintenance of good health and treatment of disease (Poorman 2001). It can also be used to describe exercise in warm water under supervision by utilizing the buoyancy, assistance and resistance of warm water to relieve pain, induce muscle relaxation, and promote more effective exercise. Hydrotherapy provides a safe and effective means of achieving exercise-related goals and is commonly used in rehabilitation programs (Al- Qubaeissy 2013). It has been utilized since ancient times in Greek medicine (Papavramidou 2003). Nowadays, hydrotherapy is used by numerous health care practitioners for various health conditions including rheumatoid arthritis (RA), osteoarthritis (OA), fibromyalgia, chronic heart failure (CHF), immune conditions, menopausal symptoms, exercise recovery, and for pain reduction (Geytenbeek 2002, Versey 2013).
The mechanisms of action of hydrotherapy treatments depend on the type of protocol used. In general, hot treatments increase perspiration, metabolism, capillary pressure, and cell permeability. Heat causes an increased demand for nutrients as well as local vasodilation and hyperemia. In addition, collateral blood circulation is enhanced (Nadler 2004). The resulting therapeutic actions include muscle relaxation, enhanced collagen flexibility, pain reduction, and anti-inflammatory actions. The effects of cold temperatures generally include an analgesic effect due to acute anti-inflammatory actions as well as potentially decreasing muscle spasms (Nadler 2004). Hydrotherapy can also cause local vasoconstriction followed by reflexive vasodilation that activates cutaneous circulation. The byproducts of metabolically active cells are vasodilators such as carbon dioxide (Fathi 2011). There is a wide range in the quality of studies available for the varying uses of hydrotherapy treatments. In general the evidence is rather limited, rendering the interpretation of existing evidence even more important. This review article will outline the available evidence for the most common uses of hydrotherapy and highlight important clinical implications.
Rheumatoid Arthritis and Osteoarthritis
The effects of hydrotherapy for RA were investigated in 139 patients with chronic RA using a four category parallel design: hydrotherapy, seated immersion, land exercise or progressive relaxation (Hall 1996). For four consecutive weeks, twice a week, participants took part in 30 minutes of intervention under the supervision of physiotherapists. This study used a variety of assessment tools on three occasions including before and after the hydrotherapy treatment and at a 3-month follow up. Assessment parameters included physical abilities, pain, and health status measures using indices to assess joint tenderness, morning stiffness, grip strength, active range of motion, as well as C-reactive protein, the Beliefs in Pain Control Questionnaire, the McGill Pain Questionnaire, and the Arthritic Impact Measurements. It was found that regardless of the intervention all patients showed significant improvement in joint tenderness between pre and post-test, with the hydrotherapy group demonstrating the greatest reduction, with a mean decrease of 27% between pre and post-test. Females in the hydrotherapy group significantly increased knee range of motion by 6.6°. This improvement was maintained at follow up, but was no longer statistically significant. Other physical measures did not change significantly. All patients experienced a significant reduction in their evaluative and affective pain scores between pre and post-tests, however this was not maintained at follow up (Hall 1996).
More recently, a systematic review examined the effectiveness of hydrotherapy in treating RA (Al- Qubaeissy 2013). In this systematic review, a total of 197 studies were identified and narrowed to six randomized controlled studies after applying specific inclusion and exclusion criteria. The reviewed studies included 419 participants both male and female with an age range of 18-80 who obtained some sort of water-based treatment, including hydrotherapy pools and aquatic exercise routines. It was determined that patients who received hydrotherapy for treatment of RA gained some beneficial effects in improving their health status and reducing their pain scores compared to the control groups, as well as joint tenderness, mood and tension symptoms, and increasing grip strength. Benefits also included a substantial increase in the physical activity and emotional well-being of patients involved in the aquatic programs. However, the long-term benefits in this study were found to be inconclusive (Al-Qubaeissy 2013). In total, the evidence suggests that hydrotherapy can improve the quality of life of RA patients as well as multiple physical and emotional measures.
The literature on hydrotherapy and OA tends to focus on treatments that include exercises in a body of water, part of the rationale being that the weight-relieving properties of water immersion allow for easier joint movement. One study compared two groups using hydrotherapy pool exercises versus similar exercises on land. This study showed that the hydrotherapy group experienced statistically significant improvements in their functional ability and had decreased pain, at least in the short-term (Sylvester 1990). A more recent randomized controlled trial included 152 older persons with chronic, symptomatic OA of the hip or knee. Participants were randomly allocated to hydrotherapy classes, Tai Chi classes, or a waiting list control group for twelve weeks. It was found that at twelve weeks, participants allocated to hydrotherapy classes demonstrated improvements for pain and physical function scores, compared with controls (Fransen 2007).
Lastly, a pilot study has also been conducted comparing the effect of hydrotherapy versus conventional physiotherapy. In this particular study, thirty patients diagnosed with symptomatic OA of the hip or knees were randomly assigned to a hydrotherapy group, a physiotherapy group, or both, for two weeks. The hydrotherapy group received daily alternate thigh affusions (pouring water). The results showed that at a 10-week follow up, the hydrotherapy group had the most beneficial effects on pain intensity and mobility (Schencking 2013). Interestingly, hydrotherapy has strong evidence supporting its use in other musculoskeletal conditions with pain, including fibromyalgia (McVeigh 2008).
Immune-Stimulation
Hydrotherapy is often described as an immune-stimulating therapy and appears to have positive effects on immunoregulation, including increases in resistance and facilitated activation of cell-mediated immune reactions (Schencking 2013). The evidence available focuses on the effects of hydrotherapy for the common colds. An older study examined the immune effects of hydrotherapy, hyperthermic exposure in particular, on the incidence of common colds (Ernst 1990). Two groups of participants were utilized. The first group was submitted to sauna bathing consisting of a warm shower, drying, eight to 12 minutes of time spent in the sauna room, and 15 minutes of cooling with cold water and resting, repeated two or three times. The second group abstained from this procedure. In both groups, the frequency, duration, and severity of common colds were recorded for six months. The results showed that there were significantly fewer episodes of common cold in the sauna group, particularly in the last three months of the study period when the incidence was approximately half compared to controls. However, the mean duration and average severity did not differ significantly between groups and the authors concluded that further research is needed (Ernst 1990).
A more recent and better designed, study examined whether or not hydrotherapy would be effective in the prevention and treatment of common colds in children (Gruber 2003). Children aged three to seven years with six or more common cold episodes during the previous year were randomized to receive daily inhalation of normal saline in the control group, or daily inhalation plus daily hydrotherapy in the experimental group for one year. The daily hydrotherapy treatment consisted of alternating warm (39°C over 10 minutes) and cold (15°C over 10 to 30 seconds). The main outcome measures were incidence, duration, and severity of common cold episodes as reported by the children’s parents in a daily symptom diary. The results showed that during the study period there were no significant differences in the incidence of colds or the average duration of episodes (Gruber 2003). This evidence suggests that hydrotherapy is therefore not an effective option for treating the common cold.

Although hydrotherapy may not be effective in treating the common cold, it may provide other immunological benefits. An in vivo study examined the immunological effects of warm and cold water exposure in mouse models (Kalenova 2005). When mice were exposed to warm or cold water, the activities of nonspecific resistance factors (peritoneal macrophages) increased upon first exposure, decreased for the following three exposures, and then increased after the fifth exposure. In particular, exposure to cold water activated cellular immunity, while warm water activated humoral immunity. The temperature alterations going from cold to warm led to the activation of cellular components and to the suppression of the humoral components of the immune system. However, the alteration of water temperature from warm to cold led to activation of nonspecific resistance factors, cellular and humoral immunity (Kalenova 2005). Many practitioners who use contrast hydrotherapy advocate ending any treatment with cold exposure. For the purposes of immune-stimulation, the evidence also favours this protocol.
Heart Failure
Hydrotherapy as part of a rehabilitation program for patients with CHF has previously been thought to be potentially dangerous due to the increased venous return caused by the hydrostatic pressure, or the changes in circulation due to the changes in fluid dynamics. However, one study found that physical training in warm water was well tolerated, improved exercise capacity as well as muscle function, with no accompanying adverse effects (Cider 2003). The New York Heart Association (NYHA) assesses the stages of heart failure (I to IV or from mild to more severe) according to a functional classification based on patient symptoms. Twenty-five patients with stable CHF (NYHA grade II–III, age 72.1 +/- 6.1 years) were randomized to either eight weeks of hydrotherapy (n = 15) or into a control group (n = 10). The experimental group training program comprised of 45 minute sessions in a heated pool (33–34°C) three times a week, following a low to moderate exercise level (40-70% max heart rate). Patients in the hydrotherapy group showed a greater improvement in their maximal exercise capacity, maximal oxygen uptake, and six-minute walk test compared to the control group (Cider 2003). Specifically, they had improvements in isometric endurance in knee extension (+4 vs. -9, p=0.01) and improvement in the performance of heel-life (+4 vs. -3 n.o, p<0.01), shoulder abduction (+12 vs. -8 s, p=0.01) and shoulder flexion (+6 vs. +4, p=0.01) (Cider 2003).

Another study looked at the addition of hydrotherapy to endurance training in elderly male patients with CHF and found a significant improvement in exercise tolerance and hemodynamic profiles (Caminiti 2011). Twenty-one male CHF patients (NYHA II-III, age 68 +/- 7 years) were randomized into two groups: 11 patients in the combined group of endurance training and hydrotherapy, and 10 patients in an endurance training only group. Hydrotherapy took place three times per week in an upright position in water at a temperature of 31°C. The treatment protocol involved callisthenic movements of the torso and both upper and lower limbs, gradually increasing from one to three sets of ten repetitions. The endurance training involved performing the same movements on land and also included 10 minutes of warm up and cool-down exercises and thirty minutes of aerobic exercise (60-70% VO2 max). At the initiation of the program and after 24 weeks all participants underwent a battery of tests including a six-minute walking test, assessment of blood pressure and heart rate, an echocardiogram, a non-invasive hemodynamic evaluation, and maximal voluntary contraction of quadriceps test. The results showed that distance in the six-minute walking test improved in both groups, but with significant intergroup differences in favour of hydrotherapy (hydrotherapy group: 150+/-32 m; control group: 105+/-28 m). Diastolic blood pressure and heart rate significantly decreased in the hydrotherapy group, but remained unchanged in the control group (−11 mm Hg+/−2, p = 0.04 and -12 beats per minute, p = 0.03; respectively). Overall, the exercise was well tolerated with no adverse effects reported (Caminiti 2011). In treating heart failure, hydrotherapy, at least delivered as exercise in warm water, appears to be a safe and effective
Another study looked at the addition of hydrotherapy to endurance training in elderly male patients with CHF and found a significant improvement in exercise tolerance and hemodynamic profiles (Caminiti 2011). Twenty-one male CHF patients (NYHA II-III, age 68 +/- 7 years) were randomized into two groups: 11 patients in the combined group of endurance training and hydrotherapy, and 10 patients in an endurance training only group. Hydrotherapy took place three times per week in an upright position in water at a temperature of 31°C. The treatment protocol involved callisthenic movements of the torso and both upper and lower limbs, gradually increasing from one to three sets of ten repetitions. The endurance training involved performing the same movements on land and also included 10 minutes of warm up and cool-down exercises and thirty minutes of aerobic exercise (60-70% VO2 max). At the initiation of the program and after 24 weeks all participants underwent a battery of tests including a six-minute walking test, assessment of blood pressure and heart rate, an echocardiogram, a non-invasive hemodynamic evaluation, and maximal voluntary contraction of quadriceps test. The results showed that distance in the six-minute walking test improved in both groups, but with significant intergroup differences in favour of hydrotherapy (hydrotherapy group: 150+/-32 m; control group: 105+/-28 m). Diastolic blood pressure and heart rate significantly decreased in the hydrotherapy group, but remained unchanged in the control group (−11 mm Hg+/−2, p = 0.04 and -12 beats per minute, p = 0.03; respectively). Overall, the exercise was well tolerated with no adverse effects reported (Caminiti 2011). In treating heart failure, hydrotherapy, at least delivered as exercise in warm water, appears to be a safe and effective conjunctive treatment.
Conclusion
Hydrotherapy is the use of water for therapeutic purposes, most commonly involving exposure to hot and cold temperatures. Though the exact mechanisms vary, there is usually an element of local vasoconstriction followed by reflexive vasodilation that activates cutaneous circulation. These physiological effects have therapeutic consequences including pain reduction and a reduction in inflammation. Hydrotherapy also appears to have positive effects on immunoregulation, including increases in resistance and facilitated activation of cell-mediated immune reactions. As discussed, many acute and chronic health conditions can potentially benefit from these effects.
Since it is limited, the evidence available with regards to effectiveness must be interpreted with caution. Hydrotherapy was shown to be effective for both RA and OA, causing reductions in pain, increased mobility, and improved quality of life. The evidence reviewed here showed that hydrotherapy was not effective in reducing the incidence, duration, or severity of the common cold in children, but that it may have other immune-stimulating effects. For patients suffering from CHF, hydrotherapy improved exercise tolerance and the hemodynamic profiles of patients, including beneficial reductions in blood pressure and heart rate. The large majority of the studies available on hydrotherapy suggest that it is a safe and effective treatment option for various health conditions.

References
Al- Qubaeissy KY, Fatoye FA, Goodwin PC, Yohannes AM. The effectiveness of hydrotherapy in the management of rheumatoid arthritis: a systematic review. Musculoskeletal Care. 2013; 11(1):3-18.
Caminiti G, Arisis A, Cerrito A, Marazzi G, Massaro R, Rosano G, Sposato B, Maurizio V. Hydrotherapy added to endurance training versus endurance training alone in elderly patients with chronic heart failure: A randomized pilot study. Int J Cardiol. 2011; 148(2):199-203.
Cider A, Schaufelberger M, Sunnerhagen K, Anderson B. Hydrotherapy- a new approach to improve function in the older patient with chronic heart failure. Eur Heart J. 2003; 5(4):527-35.
Ernst E, Pecho E, Wirz P, Saradeth T. Regular sauna bathing and the incidence of common colds. Ann Med. 1990; 22(4):225- 7.
Fathi A, Yang C, Bakhtian K, Qi M, Lonser R, Pluta R. Carbon dioxide influence on nitric oxide production in endothelial cells and astrocytes: Cellular mechanisms. Brain Res. 2011; 1386:50-57.
Fransen M, Lam P, Nairn L, Winstanly J, Edmonds J. Physical activity for osteoarthritis management: a randomized controlled clinical trial evaluating hydrotherapy or Tai Chi classes. Arthritis Rheum. 2007; 57(3): 407-14.
Geytenbeek J. Evidence for Effective Hydrotherapy. Physiotherapy. 2002; 88(9):514-29.
Gruber C, Riesberg A, Mansmann U, Knipschild P, Wahn U, Buhring M. The effect of hydrotherapy on the incidence of common cold episodes in children: a randomised clinical trial. Eur J Pediatr. 2003; 162(3):168-76.
Hall J, Skevington SM, Maddison PJ, Chapman K. A randomized and controlled trial of hydrotherapy in rheumatoid arthritis. Arthritis Care Res. 1996; 9(3):206-15.
Kalenova LF, Sukhovei YG, Fisher TA. Specific and nonspecific reactions of mouse immune system under the effect of short-term exposure in warm and/or cold water. Bull Exp Biol Med. 2005; 140(6):720-2.
McVeigh JG, McGaughey H, Hall M, Kane P. The effectiveness of hydrotherapy in the management of fibromyalgia syndrome: a systematic review. Rheumatoid Int. 2008; 29(2):119-30.
Nadler SF, Weingand K, Kruse RJ. The physiological basis and clinical application of cryotherapy and thermotherapy for the pain practitioner. Pain Physician. 2004; 7(3):395-9.
Papavramidou N, Christopoulou-Aletra H. Hydrotherapy: nineteenth century Greek scientific views. J Alt Compliment Med. 2003; 9(3):341–4.
Poorman D, Kim L, Mittman P. Naturopathic Medical Education: Where Conventional, Complementary, and Alternative Medicine Meet. Comp Health Prac Rev. 2001; 7(2):99-109.
Schencking M, Wilm S, Redaelli M. A comparison of Kneipp hydrotherapy with conventional physiotherapy in the treatment of osteoarthritis: a pilot trial. J Integr Med. 2013; 11(1):17-25.
Sylvester K. Investigation of the effect of hydrotherapy in the treatment of osteoarthritic hips. Clinical Rehab. 1990; 19890(4):223-28.
Versey NG, Halso SL, Dawson BT. Water Immersion Recovery for Athletes: Effect on Exercise Performance and Practical Recommendations. Sports Med. 2013.
FODMAP diet

FODMAP diet
Implications in irritable bowel syndrone B
Abstract
Most patients with IBS link their symptoms to food consumption. However, the current dietary recommendations for the management of IBS are inconsistent. FODMAPs, a group of short-chain carbohydrates have been identified as aggravating factors in patients with IBS. The constituents under the FODMAP umbrella are discussed. Research exploring the benefit of implementing a low FODMAP diet in patients with IBS is outlined. Recommending a reduction or an elimination of these specific carbohydrates in the diet may provide relief to those suffering with IBS.
Introduction Irritable bowel syndrome (IBS) is a common disease encountered worldwide (Morcos 2009), with a prevalence in Europe and North America between 10-15% (Hungin 2003, Quigley 2009). Typically characterized by either Rome or Manning criteria, irritable bowel syndrome is a chronic, recurring gastrointestinal problem, characterised by abdominal pain, bloating, and changes in bowel habit. Diagnosis is made by exclusion of other causes of organic bowel disease. IBS has a female predominance, often aggregating in families (Spiller 2007), with genetic studies show a connection (Hotoleanu 2008, Saito 2005).
IBS is not associated with an increase in the development of any serious diseases, however patients with IBS suffer from a reduced quality of life, both physically and mentally (Li 2003). Kennedy and Jones (2000) showed that patients with IBS are more likely to undergo surgical operations, including hysterectomy (Kennedy 2000) and cholecystectomy (Kennedy 2000). The financial burden of IBS can be quite significant due to increased medical office visits, diagnostic testing, pharmacotherapy, and emergency room visits (Martin 2001).
Many factors have been hypothesized as playing a role in the pathogenesis of IBS, including, but not limited to; gutbrain axis dysfunction (Bonaz 2009), impaired gut barrier, altered microflora, and low grade immune activation (Cremon 2009). Food intolerances are well known to play a role in the development of IBS symptoms, with patients indentifying a number of different categories of foods like those rich in carbohydrates, as well as fatty foods (Bohn 2013), coffee, alcohol, spicy food (Simren 2001), dairy (Vernia 2004), and gluten (Vazquez-Roque 2013), as common culprits. Between half and two thirds of patients with IBS associate symptoms with eating a meal (Ragnarsson 1998), with gas and abdominal pain as the most frequently reported symptoms (Simren 2001). Implementing elimination diets can be useful, but often patients don’t achieve a significant reduction in symptoms, or during the re-introduction or challenge phase, end up confused with some food reactions, due to the complex mixtures of foods, and timing (Barrett 2012).
Since IBS is so widespread, with multi-factorial causes, and varying consequences, much interest has been paid to finding ways to reduce symptoms and improve the quality of life in sufferers. Despite the lack of conclusive findings of a link between food and IBS, encouraging evidence has prompted further study of dietary modifications.
FODMAP concept and constituents
FODMAP is a relatively new concept, with the phrase being coined by a group of Australian researchers who studied the effects of a seemingly unrelated group of carbohydrates on symptoms of IBS (Gibson 2005, Shepherd 2006). FODMAP stands for fermentable oligosacchardies, disaccharides, monosaccharies, and polyols. The included short chain carbohydrates are fructose, lactose, fructo- and galactooligosaccharides (fructans, and galactans), and polyols (such as sorbitol). The acronym includes short-chain carbohydrates that are poorly absorbed and rapidly fermented, as this is the mechanism by which these carbohydrates induce symptoms. FODMAPs have also been found to be osmotically active (Barrett 2010).
The idea that fructose aggravates digestive system function is not new. Fructose is found in the diet as a free monosaccharide, hexose, as a constituent of the disaccharide sucrose, or in a polymerized form (fructan) (Gibson 2007). A study conducted in 1978 showed that fructose ingestion aggravated abdominal symptoms, and complete elimination of fructose improved symptoms of abdominal pain and colic (Andersson 1978) Absorptive capacity of fructose varies among individuals (Truswell 1988). Free fructose is absorbed by a different transport system than glucose, namely GLUT-5 (Burant 1992), which works more slowly and can be overwhelmed by large amounts of fructose (Truswell 1988). Malabsorption of fructose in healthy individuals, identified by a positive hydrogen breath test, was found in 53% of subjects given a dose of 25 grams, and in 73% of subjects given 50 grams (Beyer 2005). Despite positive breath tests, participants in the study experienced minimal gastrointestinal effects, however, studies have shown that the development of symptoms of fructose malabsorption occur much more readily in patients with IBS, and the use of fructose-free diets have dramatically reduced symptoms (Fernandez- Banares 1993, Goldstein 2000, Symons 1992). In 2008, Shepherd et al conducted a double-blinded, randomized, quadruple arm, placebo-controlled rechallenge trial. They found that symptoms of IBS were not adequately controlled in 70-79% of subjects who received fructose, fructans, or a mixture of the two carbohydrates in the context of diet. Aggravation of symptoms such as abdominal pain, bloating and flatulence occurred as patients were challenged with increasing doses of fructose and/or fructans. When subjects received the placebo, glucose alone, they experienced significantly less severe symptoms, which suggests that dietary restriction of fructose and/or fructans is likely to be responsible for symptomatic improvement.
The question of why a natural sugar found in fruit and other foods has more recently been found to cause digestive system symptoms relates to the increased intake of concentrated fructose. The development of high fructose corn syrup (containing on average 47-65% fructose (Ventura 2011)) and subsequent increase in consumption (Beyer 2005), is hypothesized to be a key factor involved in the increase in fructose malabsorption (Latulippe 2011). The average intake of fructose was thought to be approximately 37 g per day (Park 1993) but was then re-evaluated in 2004 to be 49 g/day (Marriott 2009). This increase in dietary fructose load may more commonly exceed the absorptive capacity of the intestines, exacerbating or unmasking IBS (Shepherd 2006).
Interestingly, fructose absorption is altered depending on glucose presence. As previously mentioned, the absorption mechanism for fructose as a monosaccharide via the GLUT-5 transporter can become saturated. Studies have indicated that when glucose is present, either as free glucose, or when glucose and fructose are combined to form the disaccharide, sucrose, fructose absorptive capacity is increased (Riby 1993) by up-regulation of the GLUT-2 transporter and no malabsorptive state results (Shepherd 2006). This is clinically relevant, as researchers Barrett and Shepherd indicated, because it allows patients to choose foods that are fructose and glucose balanced (e.g. berries and stone fruits) or where glucose is in greater amounts, rather than completely eliminating all fructose containing foods. Another option is to consume glucose with high fructose containing foods, however this could present a problem for blood sugar control.
Fructans are oligosaccharides and polysaccharides of fructose units with a glucose terminal end (Gibson 2007). They are referred to as inulins and fructooligosaccharides (FOS) and are found in foods such as wheat, onions, garlic, artichokes, and chicory. Fructans are completely unabsorbed by upper gastrointestinal tract, and are therefore rapidly fermentable (Rumessen 1998). Fructo-oligosaccharide is a well known prebiotic fibre, that has numerous health benefits, including its ability to increase populations of bacteria in the gut, specifically Bifidobacteria (Gibson 1995). However, research has shown that large amounts (14-20 g) of fructans can aggravate symptoms in people suffering from IBS (Olesen 2000), and can cause digestive upset (especially flatulence) even in healthy individuals (Pedersen 1997, Stone-Dorshow 1987). The average daily intake of fructans via the diet has been calculated to be as much as 10 g/day (van Loo 1995), but with the addition of inulin or FOS to food for its many health benefits, daily intake levels could be greater. Wheat, which accounts for 70% of the daily intake of fructans (Moshfegh 1999), could also be problematic, especially when consumed in large amounts. This may in part explain why gluten elimination has been found to decrease symptoms in individuals who suffer from IBS.
Like fructans, galactans, polymers of galactose, more commonly known as raffinose and styachose, are almost completely unabsorbed in all people, leading to significant fermentation and therefore gas production. Galactans are found in large amounts in legumes, including lentils, chickpeas, kidney beans and have been found to aggravate symptoms of IBS (Chirila 2012), and are therefore included under the FODMAP umbrella.
Lactose is the disaccharide included under the FODMAP umbrella. Lactose absorption depends on the activity of the hydrolase enzyme lactase, which is deficient in 2-100% of people in various populations worldwide (Swagerty 2002). Sixty-eight percent of people with IBS tested positive, via hydrogen breath test, for lactose malabsorption. After adhering to a lactose-free diet, symptoms subsided in nearly half of study participants. Other studies have found similar results (Bohmer 1996), and have suggested that the use of a hydrogen breath test could be used to identify lactose malabsorbers, thus allowing a less strict diet.
Polyols, are sugar alcohols, including; sorbitol, xylitol, mannitol, maltitol, and isomalt, found naturally in some foods and added to many foods as artificial sweeteners. Polyols are incompletely absorbed, and it is well known that sorbitol specifically, has an osmotic laxative effect at high amounts (Hyams 1983). Unlike fructose, polyols do not have an associated active transport system in the small intestine and are probably absorbed by passive diffusion (Gibson 2010). The incomplete absorption of sugar alcohols has been found in healthy controls, at larger doses, indicating a dose response to malabsorption (Corazza 1988). Despite positive hydrogen breath tests, not all malabsorbers displayed symptoms, however, those with IBS experienced significantly more symptoms (Fernandez-Banares 1993, Nelis 1990, Symons 1992)
As evident in the literature, each of the carbohydrate constituents of FODMAPs have been investigated individually. Tests of FODMAPs as a whole have also been conducted, not only by the Australian research group who originally grouped the short-chain carbohydrates together, but increasingly by other researchers worldwide and are showing promising results (Staudacher 2011, Ostgaard 2012, de Roest 2013).
The FODMAP diet in research
Mechanistically the FODMAP diet as a whole has been studied using an ileostomy model, which has been used to study the digestion and absorption of carbohydrates in previous studies (Englyst 1985, Langkilde 1994). Barrett et al (2010) investigated the effect of dietary FODMAPs on the content of water and fermentable substrates of ileal effluent. Individuals with an ileostomy, but no evidence of small intestinal disease, undertook two 4-day dietary periods, comprising diets differing only in FODMAP content. Ileal effluent was collected every two hours on day four of each diet. The FODMAP content of the diet and effluent was measured and patients rated the effluent consistency on a visual analog scale. The effluent of the high FODMAP diet was found to be greater in dry weight and water content. Study participants perceived effluent consistency to be thicker with the low FODMAP diet. The researchers concluded that FODMAPs do increase delivery of water and fermentable substrates to the proximal colon (Barrett 2010). This study was the first mechanism type study that specifically addressed FODMAPs in the diet, as opposed to certain carbohydrates in isolation, confirming that FODMAPs as part of a diet are osmotically active and their poor absorption gives rise to potential fermentation and associated gas production.
It is well known that people suffering from IBS often experience abdominal pain, bloating, and gas due to luminal distension. Ong et al (2010) demonstrated that dietary manipulation of FODMAPs can impact the total amount of gastrointestinal gas production and the spectrum of gas produced (hydrogen vs. methane) in healthy individuals and those with IBS. While an increase in gas was seen even in healthy individuals ingesting a high FODMAP diet, increased gastrointestinal symptoms as well as systemic symptoms, like fatigue, were seen in patients with IBS.
A number of studies have linked the gut microenvironment with the pathophysiology of IBS (Simren 2013). Studies have identified inherent differences in the gut microflora and thus fermentation in IBS patients versus controls (Kassinen 2007, Madden 2002), which could explain the connection with FODMAPs, showing that FODMAPs don’t cause IBS, but could be aggravating symptoms by providing rapidly fermentable substrates to the intestines. Small intestine bacterial overgrowth (SIBO) has been found to be associated with IBS (Sachdeva 2011), and by nature of the FODMAP diet, a reduction in the intake of short-chain carbohydrates, and therefore fermentation, could be useful as dietary treatment.
In a recent study, 90 patients with IBS received dietary advice regarding a low FODMAP diet and completed a hydrogen/methane breath testing for fructose and lactose malabsorption (deRoest 2013). Patients were then asked to complete a questionnaire approximately 15 months later. Results revealed a significant improvement in abdominal pain, bloating, flatulence. The authors concluded that breath testing was a good way to help people understand and adhere to the diet (de Roest 2013). Breath testing has been used and recommended by other researchers as a clinical tool for assessing malabsorption (Barrett 2009, Gibson 2010). Gibson et al (2010) have suggested that breath testing for fructose and lactose malabsorption might be worthwhile because it would allow foods with negative results to be reintroduced back into the diet to a comfortable level, avoiding unnecessary restrictions(Gibson 2010), and providing a source of beneficial prebiotic fibre (Barrett 2012).
Clinical Utility
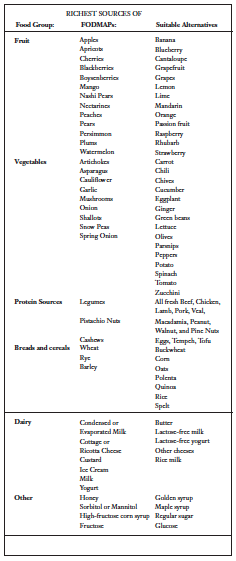
Table 1 (CCS 2012) outlines foods that are high in FODMAPs and suitable alternatives. Since food plays a large role in patient’s perception of symptom induction, many IBS sufferers are potentially already unknowingly avoiding FODMAP foods. The FODMAP diet has been shown to be fairly simple to implement, with limited instruction (Ostgaard 2012). A study by Ostgaard et al (2012) showed that after two hours of dietary guidance by a dietician, patients with IBS avoided all FODMAP‑rich food, consumed more food with probiotic supplements and did not avoid food sources that were crucial to their health. They had improved quality of life and reduced symptoms. Guidance on the management of diet improved their choice of a healthier diet, improved quality of life and reduced IBS symptoms.
Gibson et al (2009) suggest a strict low FODMAP diet for a period of six to eight weeks, followed by a trial of foods to test tolerance, keeping total low FODMAP intake in mind. This would allow patients to occasionally consume foods deemed high FODMAP to a tolerable level, to ensure variety in the diet.
A low FODMAP diet improved symptoms in at least 74% of patients with IBS (Barrett 2012). In the UK, The FODMAP diet was studied in comparison to the UK National Institute for Health and Clinical Excellence (NICE) dietary guidelines for symptom control in patients with IBS. Up to 86% of patients in the FODMAP group experienced overall symptom response, versus 49% in the standard group. Significantly more patients in the low FODMAP group reported improvements in bloating, abdominal pain, and flatulence. This drew the conclusion that a low FODMAP diet is more effective than the standard dietary advice in the UK, for symptom control in IBS (Staudacher 2011). With a continually growing body of evidence, both for the individual constituents of FODMAPs, as well as FODMAPs as a whole, the FODMAP diet seems a reasonable option for dietary management in patients suffering from IBS.
References
Andersson DEH, Nygren A. Four Cases of Long-Standing Diarrhoea and Colic Pains Cured by Fructose-Free diet—A Pathogenetic Discussion. Acta Medica Scandinavica. 1978;203(1- 6):87-92.
Barrett JS. Extending our knowledge of fermentable, short- chain, carbohydrates for managing gastrointestinal symptoms. Nutrition in Clinical Practice. 2013;28(3):300-306.
Barrett JS, Gearry RB, Muir JG, Irving PM, Rose R, Rosella O, Haines ML, Shepherd SJ, Gibson PR. Dietary poorly absorbed, short-chain carbohydrates increase delivery of water and fermentable substrates to the proximal colon. Aliment Pharmacol Ther. 2010 Apr;31(8): 874-882.
Barrett JS, Gibson PR. Fermentable oligosaccharides, disaccharides, monosaccharides and polyols (FODMAPs) and nonallergic food intolerance: FODMAPs or food chemicals? Therap Adv Gastroenterol. 2012 Jul;5(4): 261-268.
Barrett JS, Irving PM, Shepherd SJ, Muir JG, Gibson PR. Comparison of the prevalence of fructose and lactose malabsorption across chronic intestinal disorders. Aliment Pharmacol Ther. 2009 Jul;30(2): 165-174.
Beyer PL, Caviar EM, McCallum RW. Fructose intake at current levels in the United States may cause gastrointestinal distress in normal adults. J Am Diet Assoc. 2005 Oct;105(10): 1559-1566.
Bohmer CJ, Tuynman HA. The clinical relevance of lactose malabsorption in irritable bowel syndrome. Eur J Gastroenterol Hepatol. 1996 Oct;8(10): 1013-1016.
Bohn L, Storsrud S, Tornblom H, Bengtsson U, Simren M. Self-reported food-related gastrointestinal symptoms in IBS are common and associated with more severe symptoms and reduced quality of life. Am J Gastroenterol. 2013 May;108(5): 634-641.
Bonaz B, Sabate JM. Brain-gut axis dysfunction. Gastroenterol Clin Biol. 2009 Feb;33 Suppl 1: S48-58.
Burant CF, Takeda J, Brot-Laroche E, Bell GI, Davidson NO. Fructose transporter in human spermatozoa and small intestine is GLUT5. J Biol Chem. 1992 Jul;267(21): 14523-14526.
CCS, Monash University. The Monash University Low FODMAP Diet. 2012. Melbourne, Australia, Monash University.
Chirila I, Petrariu FD, Ciortescu I, Mihai C, Drug VL. Diet and irritable bowel syndrome. J Gastrointestin Liver Dis. 2012 Dec;21(4): 357-362.
Corazza GR, Strocchi A, Rossi R, Sirola D, Gasbarrini G. Sorbitol malabsorption in normal volunteers and in patients with coeliac disease. Gut. 1988 Jan;29(1): 44-48.
Cremon C, Gargano L, Morselli-Labate AM, Santini D, Cogliandro RF, De Giorgio R, Stanghellini V, Corinaldesi R, Barbara G. Mucosal immune activation in irritable bowel syndrome: gender-dependence and association with digestive symptoms. Am J Gastroenterol. 2009 Feb;104(2): 392-400.
de Roest RH, Dobbs BR, Chapman BA, Batman B, O’Brien LA, Leeper JA, Hebblethwaite CR, Gearry RB. The low FODMAP diet improves gastrointestinal symptoms in patients with irritable bowel syndrome: a prospective study. Int J Clin Pract. 2013 May;epub.
Englyst HN, Cummings JH. Digestion of the polysaccharides of some cereal foods in the human small intestine. The American Journal of Clinical Nutrition. 1985 Nov;42(5): 778-787.
Fernandez-Banares F, Esteve-Pardo M, de Leon R, Humbert P, Cabre E, Llovet JM, Gassull MA. Sugar malabsorption in functional bowel disease: clinical implications. Am J Gastroenterol. 1993 Dec;88(12): 2044-2050.
Gibson GR, Beatty ER, Wang X, Cummings JH. Selective stimulation of bifidobacteria in the human colon by oligofructose and inulin. Gastroenterology. 1995 Apr;108(4): 975-982.
Gibson PR, Newnham E, Barrett JS, Shepherd SJ, Muir JG. Review article: fructose malabsorption and the bigger picture. Aliment Pharmacol Ther. 2007 Feb;25(4): 349-363.
Gibson PR, Shepherd SJ. Personal view: food for thought–western lifestyle and susceptibility to Crohn’s disease. The FODMAP hypothesis. Aliment Pharmacol Ther. 2005 Jun;21(12): 1399- 1409.
Gibson PR, Shepherd SJ. Evidence-based dietary management of functional gastrointestinal symptoms: The FODMAP approach. J Gastroenterol Hepatol. 2010 Feb;25(2): 252-258.
Goldstein R, Braverman D, Stankiewicz H. Carbohydrate malabsorption and the effect of dietary restriction on symptoms of irritable bowel syndrome and functional bowel complaints. Isr Med Assoc J. 2000 Aug;2(8): 583-587.
Hotoleanu C, Popp R, Trifa AP, Nedelcu L, Dumitrascu DL. Genetic determination of irritable bowel syndrome. World J Gastroenterol. 2008 Nov;14(43): 6636-6640.
Hungin AP, Whorwell PJ, Tack J, Mearin F. The prevalence, patterns and impact of irritable bowel syndrome: an international survey of 40,000 subjects. Aliment Pharmacol Ther. 2003 Mar;17(5): 643-650.
Hyams JS. Sorbitol intolerance: an unappreciated cause of functional gastrointestinal complaints. Gastroenterology. 1983 Jan;84(1): 30-33.
Kassinen A, Krogius-Kurikka L, Makivuokko H, Rinttila T, Paulin L, Corander J, Malinen E, Apajalahti J, Palva A. The fecal microbiota of irritable bowel syndrome patients differs significantly from that of healthy subjects. Gastroenterology. 2007 Jul;133(1): 24-33.
Kennedy TM, Jones RH. Epidemiology of cholecystectomy and irritable bowel syndrome in a UK population. Br J Surg. 2000 Dec;87(12): 1658-1663.
Kennedy TM, Jones RH. The epidemiology of hysterectomy and irritable bowel syndrome in a UK population. Int J Clin Pract. 2000 Dec;54(10): 647-650.
Langkilde AM, Andersson H, Schweizer TF, Wursch P. Digestion and absorption of sorbitol, maltitol and isomalt from the small bowel. A study in ileostomy subjects. Eur J Clin Nutr. 1994 Nov;48(11): 768-775.
Latulippe ME, Skoog SM. Fructose malabsorption and intolerance: effects of fructose with and without simultaneous glucose ingestion. Crit Rev Food Sci Nutr. 2011 Aug;51(7): 583- 592.
Li FX, Patten SB, Hilsden RJ, Sutherland LR. Irritable bowel syndrome and health-related quality of life: a population-based study in Calgary, Alberta. Can J Gastroenterol . 2003 Apr;17(4): 259-263.
Madden JA, Hunter JO. A review of the role of the gut microflora in irritable bowel syndrome and the effects of probiotics. Br J Nutr. 2002 Sep;88 Suppl 1:S67-72.
Marriott BP, Cole N, Lee E. National estimates of dietary fructose intake increased from 1977 to 2004 in the United States. J Nutr. 2009 Jun;139(6): 1228S-1235S.
Martin R, Barron JJ, Zacker C. Irritable bowel syndrome: toward a cost-effective management approach. Am J Manag Care. 2001 Jul;7(8 Suppl): S268-275.
Morcos A, Dinan T, Quigley EM. Irritable bowel syndrome: role of food in pathogenesis and management. J Dig Dis. 2009 Nov;10(4): 237-246.
Moshfegh AJ, Friday JE, Goldman JP, Ahuja JK. Presence of inulin and oligofructose in the diets of Americans. J Nutr. 1999 Jul;129(7 Suppl): 1407S-1411S.
Nelis GF, Vermeeren MA, Jansen W. Role of fructose-sorbitol malabsorption in the irritable bowel syndrome. Gastroenterology. 1990 Oct;99(4): 1016-1020.
Olesen M, Gudmand-Hoyer E. Efficacy, safety, and tolerability of fructooligosaccharides in the treatment of irritable bowel syndrome. Am J Clin Nutr. 2000 Dec;72(6): 1570-1575.
Ong D, Mitchell S, Barrett J, Shepherd S, Irving P, Biesiekierski J, Smith S, Gibson P, Muir J. Manipulation of dietary short chain carbohydrates alters the pattern of gas production and genesis of symptoms in irritable bowel syndrome. J Gastroenterol Hepatol. 2010 Aug;25(8): 1366-1373.
Ostgaard H, Hausken T, Gundersen D, El-Salhy M. Diet and effects of diet management on quality of life and symptoms in patients with irritable bowel syndrome. Mol Med Rep. 2012 Jun;5(6): 1382-1390.
Park YK, Yetley EA. Intakes and food sources of fructose in the United States. Am J Clin Nutr. 1993 Nov;58(5 Suppl): 737S-747S.
Pedersen A, Sandstrom B, Van Amelsvoort JM. The effect of ingestion of inulin on blood lipids and gastrointestinal symptoms in healthy females. Br J Nutr. 1997 Aug;78(2): 215-222.
Quigley E, Fried M, Gwee KA, Olano C, Guarner F, Khalif I, Hungin P, Lindberg G, Abbas Z, Bustos- Fernandez L, Mearin F, Bhatia SJ, Hu PJ, Schmulson M, Krabshuis JH, Le Mair AW. Irritable bowel syndrome: a global perspective. 2009. W. G. O. G. Guideline.
Ragnarsson G, Bodemar G. Pain is temporally related to eating but not to defaecation in the irritable bowel syndrome (IBS). Patients’ description of diarrhea, constipation and symptom variation during a prospective 6-week study. Eur J Gastroenterol Hepatol. 1998 May;10(5): 415-421.
Riby JE, Fujisawa T, Kretchmer N. Fructose absorption. Am J Clin Nutr. 1993 Nov;58(5): 748S-753S.
Rumessen JJ, Gudmand-Hoyer E. Fructans of chicory: intestinal transport and fermentation of different chain lengths and relation to fructose and sorbitol malabsorption. Am J Clin Nutr. 1998 Aug;68(2): 357-364.
Sachdeva S, Rawat AK, Reddy RS, Puri AS. Small intestinal bacterial overgrowth (SIBO) in irritable bowel syndrome: frequency and predictors. J Gastroenterol Hepatol. 2011 Apr;26 Suppl 3: 135-138.
Saito YA, Petersen GM, Locke GR, Talley NJ. The genetics of irritable bowel syndrome. Clin Gastroenterol Hepatol. 2005 Nov;3(11): 1057- 1065.
Shepherd S J, Gibson PR. Fructose malabsorption and symptoms of irritable bowel syndrome: guidelines for effective dietary management. J Am Diet Assoc. 2006 Oct;106(10): 1631-1639.
Shepherd SJ, Parker FC, Muir JG, Gibson PR. Dietary triggers of abdominal symptoms in patients with irritable bowel syndrome: randomized placebo-controlled evidence. Clin Gastroenterol Hepatol. 2008 Jul;6(7): 765-771.
Simren M, Barbara G, Flint HJ, Spiegel BM, Spiller RC, Vanner S, Verdu EF, Whorwell PJ, Zoetendal EG. Intestinal microbiota in functional bowel disorders: a Rome foundation report. Gut. 2013 Jan;62(1): 159-176.
Simren M, Mansson A, Langkilde AM, Svedlund J, Abrahamsson H, Bengtsson U, Bjornsson ES. Food-related gastrointestinal symptoms in the irritable bowel syndrome. Digestion. 2001;63(2): 108-115.
Spiller R, Aziz Q, Creed F, Emmanuel A, Houghton L, Hungin P, Jones R, Kumar D, Rubin G, Trudgill N, Whorwell P. Guidelines on the irritable bowel syndrome: mechanisms and practical management. Gut. 2007 Dec;56(12): 1770-1798.
Staudacher HM, Whelan K, Irving PM, Lomer MC. Comparison of symptom response following advice for a diet low in fermentable carbohydrates (FODMAPs) versus standard dietary advice in patients with irritable bowel syndrome. J Hum Nutr Diet. 2011 Oct;24(5): 487-495.
Stone-Dorshow T, Levitt MD. Gaseous response to ingestion of a poorly absorbed fructo-oligosaccharide sweetener. Am J Clin Nutr. 1987 Jul;46(1): 61-65.
Swagerty DL, Jr., Walling AD, Klein RM. Lactose intolerance. Am Fam Physician. 2002 May;65(9): 1845-1850.
Symons P, Jones MP, Kellow JE. Symptom provocation in irritable bowel syndrome. Effects of differing doses of fructose-sorbitol. Scand J Gastroenterol. 1992 Nov;27(11): 940-944.
Truswell AS, Seach JM, Thorburn AW. Incomplete absorption of pure fructose in healthy subjects and the facilitating effect of glucose. Am J Clin Nutr. 1988 Dec;48(6): 1424-1430.
van Loo J, Coussement P, de Leenheer L, Hoebregs H, Smits G. On the presence of inulin and oligofructose as natural ingredients in the western diet. Crit Rev Food Sci Nutr. 1995 Nov;35(6): 525-552.
Vazquez-Roque MI, Camilleri M, Smyrk T, Murray JA, Marietta E, O’Neill J, Carlson P, Lamsam J, Janzow D, Eckert D, Burton D, Zinsmeister AR. A controlled trial of gluten-free diet in patients with irritable bowel syndrome-diarrhea: effects on bowel frequency and intestinal function. Gastroenterology. 2013 May;144(5): 903-911 e903.
Ventura EE, Davis JN, Goran MI. Sugar content of popular sweetened beverages based on objective laboratory analysis: focus on fructose content. Obesity (Silver Spring). 2011 Apr;19(4): 868-874.
Vernia P, Marinaro V, Argnani F, Di Camillo M, Caprilli R. Selfreported milk intolerance in irritable bowel syndrome: what should we believe? Clin Nutr. 2004 Oct;23(5): 996-1000.





