





An expert panel found that 16 freely accessible online tests for Alzheimer’s disease scored poorly on scales of overall scientific validity, reliability and ethical factors, according to new data reported at the Alzheimer’s Association International Conference® 2013 (AAIC® 2013) in Boston. “As many as 80 percent of Internet users, including a growing proportion of older adults, seek health information and diagnoses online,” said Julie Robillard, Ph.D., a postdoctoral fellow at the National Core for Neuroethics at the University of British Columbia in Vancouver, British Columbia, Canada, who presented the data at AAIC 2013. “Self-diagnosis behavior in particular is increasingly popular online, and freely accessible quizzes that call themselves ‘tests’ for Alzheimer’s are available on the Internet. However, little is known about the scientific validity and reliability of these offerings and ethics-related factors including research and commercial conflict of interest, confidentiality and consent. Frankly, what we found online was distressing and potentially harmful,” Robillard added. According to the Alzheimer’s Association 2013 Alzheimer’s Disease Facts and Figures report, more than five million Americans are living with Alzheimer’s disease. By 2050, the number of people with Alzheimer’s could reach 13.8 million. Other estimates suggest that number could be high as 16 million. “The number of people with Alzheimer’s is projected to rise significantly as more and more people age into greater risk for developing the disease,” said Maria Carrillo, Ph.D., Alzheimer’s Association vice president of medical and scientific Relations. “Especially in that context, active promotion of healthy aging is a priority for the Alzheimer’s Association, as is the delivery of accurate, reliable and ethical information and services.” All 16 tests scored “poor” or “very poor” on the evaluation criteria for ethical factors. According to Robillard, ethical issues with the tests included overly dense or absent confidentiality and privacy policies, failure to disclose commercial conflicts of interests, failure to meet the stated scope of the test and failure to word the test outcomes in an appropriate and ethical manner.
Poverty the Greatest Barrier to Good Health, Canadians tell CMA Consultation
Poverty kills. That’s the key message in What Makes us Sick, a report released today by the Canadian Medical Association (CMA) based on what Canadians said during a series of town hall meetings and an online consultation held earlier this year. The national dialogue with Canadians asked them about their experiences with the social determinants of health – the factors that cause people to suffer poor health in the first place. “Many factors outside the health care system affect a person’s health, from inadequate housing to a lack of healthy food to sub-optimal early childhood experiences,” said Dr. Anna Reid, past CMA president. “What Canadians told us is that poverty is the recurring theme that underpins most of these social determinants of health.” The CMA report included recommendations for action, again, based on what Canadians said. However, Dr. Reid stressed that the report does not lay blame. “We aren’t pointing fingers,” she said. “We listened to Canadians and what we heard was that they want sincere, legitimate and real action. As a country we can do better in tackling issues around poverty, housing, early childhood development, food security and culture that can hinder a person’s chances to be healthy. There is no one sector responsible for making this happen. It has to be a joint effort, involving health care providers, governments, patients and Canadians from all backgrounds.”
CMA Recognizes Excellence in the Field of Medical Ethics
The Canadian Medical Association (CMA) announced that Dr. David McKnight of Toronto and Dr. Ian Mitchell of Calgary will receive the 2013 Dr. William Marsden Award in Medical Ethics. This award recognizes CMA members who have demonstrated exemplary leadership, commitment and dedication to the cause of advancing and promoting excellence in the field of medical ethics in Canada. Dr. David McKnight is widely admired for his leadership and dedication to excellence in the field of medical ethics. He began teaching ethics in anesthesia in 1990 and has won several awards for excellence in postgraduate education. Currently the associate dean of equity and professionalism for the faculty of medicine at the University of Toronto, he introduced the “Stethoscope Ceremony” during orientation for new medical students, symbolizing the importance of listening. He is also responsible for an empowering diversity statement for faculty recruitment. Dr. Ian Mitchell is a leader who enhances ethical and professional behaviour in physicians and displays excellence in his own ethics research and teaching initiatives. He is known as a meta-teacher who serves bioethics and the profession with insight, innovation and fearlessness. “I was honoured to be nominated and overwhelmed to be granted this award,” said Dr. Mitchell. “It is a privilege to work with children and families, and to encourage aspiring physicians to consider all aspects of care. Ethics are integral to the best health care.” After studying medicine at the University of Edinburgh, Dr. Mitchell pursued specialty training in pediatrics and pediatric lung disease. In 1982 he accepted a position at Alberta Children’s Hospital and joined the faculty of the University of Calgary’s department of paediatrics. Currently holding the rank of professor, he is director of the Respiratory Home Care Clinic.
Large-Scale Cost-Effectiveness Study of Non-Invasive Prenatal Testing in Canada
A team of researchers led by CHU de Quebec and Universite Laval, has received CAN$10.5 million from Genome Canada, the Canadian Institutes of Health Research (CIHR), Genome Quebec and other partners to conduct a large-scale comparative effectiveness study on non-invasive prenatal screening techniques. Dr. Francois Rousseau and his team will examine current prenatal screening practices for chromosomal conditions, such as Down syndrome, among pregnant women in Canada in order to improve screening approaches and avoid unnecessary procedures. Each year in Canada, about 450,000 women become pregnant and are offered Down syndrome prenatal screening using biochemical and ultrasound markers. The vast majority will be negative or low risk. However, for positive or high-risk results, those pregnant women are referred to amniocentesis, which is an invasive procedure done to confirm the screening result. Approximately 5% of all biochemical screening results are falsely positive, attributing to unnecessary invasive procedures that pose a 1 in 300 risk for miscarriage. The research project aims at independently comparing the performances of different such approaches that involve various combinations of the available tools for screening of chromosomal conditions, as well as to evaluate the cost-effectiveness, the ethical and social aspects of this new technology and to identify and adapt the best implementation tools for users in the health care system. The researchers will recruit 5600 pregnant women (3600 at high-risk of trisomy conditions and 2000 at low-risk). Samples from these women will be tested in parallel using different screening approaches that involve genomic-based NIPT, but also existing or new biochemical and ultrasound screening tools. The samples will be analyzed without knowledge of the true status of the pregnancy outcome. This will provide a comprehensive evaluation of the most efficient ways to improve the prenatal screening techniques widely used today.
Canadian Association Of Interns And Residents: 6 Practical Steps To Better Care
According to new research conducted by the Canadian Association of Interns and Residents (CAIR), Canada needs a better way to anticipate the supply and demand of physicians if we are to meet patient needs in the future. Reliable data and better coordination between patient needs and residency training positions would also help residents with career decisions, ultimately resulting in better patient care. Based on the findings of its work, the CAIR Committee adopted six Principles that would bring about a more effective way of coordinating physician health human resources across the country: Effective, evidence-based workforce planning for Canadian patients and physicians, allocation of residency training positions that aligns with population needs and job availability, particularly in specialty areas, improvements to the work environment in rural areas to attract and retain new physicians in local communities, career counseling throughout medical training, promotion of a culture of social accountability in medical training and succession planning.
Super spice saffron for Canadians concerned about eye health
Saffron, one of the most esteemed spices in the world is now being used in an eye supplement approved by Health Canada and claimed to be a new hope for individuals affected by age-related macular degeneration (AMD) and cataracts, the two leading causes of vision impairment in Canada. Studies have shown the retinal protective effects and vision improvement properties of saffron in patients with AMD. Saffron 2020 is an eye supplement that combines saffron with other nutrients known to be important for eye health, and is the only saffron-containing supplement approved by Health Canada for macular degeneration and cataracts. Saffron 2020 was formulated following studies in Italy and Australia showing the benefits of saffron in patients with AMD. This natural health product helps to maintain our invaluable eyesight in AMD and cataracts, and also helps to reduce the risk of developing cataracts. Doctor Kim Julian, a top eye surgeon involved in the elaboration of Saffron 2020, stated: “At the moment, there is no cure for AMD, all we can do is aim to slow down its progression and make life as manageable as possible for this suffering. Saffron 2020 is the only supplement I’m aware of which combines saffron with important eye health nutrients like resveratrol, zinc, antioxidant vitamins (A, B2, C and E) and natural carotenoids lutein and zeaxanthin.” Saffron 2020 is a patent pending product provided by Groupe Persavita, a company located in Montreal, Canada.
Canadians Want a National Strategy for Seniors Health Care
Nine out of 10 (93%) Canadians believe Canada needs a pan-Canadian strategy for seniors health care at home, hospitals, hospices and long-term facilities, the Canadian Medical Association’s (CMA) 2013 National Report Card on health issues has found. In addition, an equal number believe a comprehensive strategy for seniors health care would improve the entire system by keeping elderly Canadians at home as long as possible, thereby lightening the load on hospitals and long-term care facilities, the Ipsos Reid poll found. Nine out of 10 respondents (89%) believe a national strategy for seniors should involve federal, provincial, territorial and municipal levels of government. And four in five (78%) believe the federal government has an important role to play in developing the strategy. Research shows that it costs $126 a day to provide care for a patient in a long-term care facility, versus $842 a day in a hospital. Of course, making it easier for elderly Canadians to stay at home while getting the care they need would be the preferred and most cost-effective option. “The results of this year’s CMA report card send a clear and direct message to policy-makers and public office holders that all levels of government need to act to address the demographic tsunami that is heading toward the health care system,’’ said past CMA President Dr. Anna Reid. The poll, conducted between July 17 and July 26 by phone with 1,000 Canadians 18 and over, found that four in five (83%) Canadians thought their health care in retirement years was a concern. The results show a majority (63%) believe home and community care should be the most important focus for governments when improving health care quality for senior citizens.
Brain Cancer Lesion Treated with Precisely-Aimed Laser Catheter
IMRIS Inc. and MRI Interventions, Inc. announced that a surgical team at Brigham and Women’s Hospital (BWH) in Boston, MA, has performed the first laser ablation procedure to combine the use of MRI Interventions’ ClearPoint® Neuro Intervention System as the navigation platform with intraoperative MRI (iMRI) in an IMRIS VISIUS® Surgical Theatre. The combination of these two enabling technologies provided continuous visualization and guidance throughout a neurosurgical intervention to treat a right frontal brain tumor. “The combination of the two technologies made for a smooth and successful operation,” said Dr. Alexandra Golby, BWH neurosurgeon and associate professor of surgery at Harvard Medical School. “We had access to excellent real-time MR images within a hi-tech surgical suite and were able to use those images to guide and deliver the needed therapy to specific targets in the brain with a high degree of precision.” The ClearPoint navigation platform enables minimally-invasive neurosurgery under continuous MR guidance, and offers surgeons a direct view of the inside of a patient’s brain during a procedure. The VISIUS Surgical Theatre allows use of intraoperative MRI right inside the operating room and over the OR table. Using the ClearPoint system with VISIUS iMRI, Golby was able to see and select the lesion of the tumor in the brain, establish a safe trajectory, and visualize the laser catheter on MR images as it was inserted to the desired location. She was then able to utilize real-time MR thermometry to monitor progress as the laser catheter heated the target area to the desired temperature for therapeutic destruction of the malignant tissue, preserving surrounding healthy tissue in the process. MRI is the only imaging technology that will safely allow this continuous soft tissue visualization during surgery. Finally, Golby was able to confirm results of the procedure using the MRI before the patient was removed from the operating table.
Breaking it down

successful completion of the questions at the end of this paper has been approved for continuing education by the bddt-n; 1.0 credit nutritional medicine and by the cnpbc; one ce hour.
1Bachelor of Health Sciences (Honours), McMaster University. Naturopathic Doctor, Canadian College of Naturopathic Medicine
2Bachelor of Health Sciences (Honours) Candidate, McMaster University.
Breaking it down
The role of acid-base balance in the pathogenesis and treatment of osteoporosis
ABSTRACT
Osteoporosis (OP) is a skeletal disorder characterized by low bone mineral density (BMD), which predisposes individuals to increased risk of skeletal fractures (Foundation 2010). In 2009, more than 22% of Canadians over the age of 50 were diagnosed with OP (Garriguet 2011). In 2010, OP accounted for $2.3 billion in Canada’s healthcare expenditures of which over 50% were utilized for acute care of managing OP-related fractures (Tarride 2012). The etiology of OP is defined by elevated osteoclastic activity relative to osteoblastic activity, which induces bone resorption and deterioration of bone tissue (Duque 2008). OP is associated with multiple risk factors including advanced age, hormone imbalance, sedentary lifestyle, and hypocalcaemia (Tucker 2001). However, Kanis et al. (Kanis 2007) found that measuring BMD in addition to clinical risk factors provides the best fracture risk prediction.
The standard first-line therapy for OP includes oral bisphosphonates combined with vitamin D and calcium (Ca) supplementation therapy, which are recommended from the age of 50 (Papaioannou 2010). However, bisphosphonates diminish in efficacy following three to five years of treatment and may cause severe adverse effects such as osteonecrosis of the jaw (Nase 2006, Rachner 2011). As such, investigation into alternative therapies is warranted. Furthermore, the role of Ca deficiency in the pathogenesis of OP fails to account for higher rates of hip fracture in Western countries with higher Ca intake relative to developing countries with lower Ca intake (FAO 2004, Poliquin 2009). As a result, alternative factors for disease progression, including those that influence the efficacy of Ca supplementation, have been investigated (FAO 2004).
It has been suggested that a diet consisting of protein and grains is associated with an increased net acid load, which is buffered via bone dissolution (Fenton 2009a, Wachman 1968). The result is a decrease in BMD and a release of calcium from bone, which is subsequently excreted through urine (Fenton 2009a). It is posited that an alkaline diet consisting of a high intake of fruits and vegetables, which are metabolized to bicarbonate (HCO3), would buffer acidity and thereby preserve Ca levels and BMD (Fenton 2009a). The objective of this article is to explore the role of acid-base balance in OP pathogenesis, as well as its potential to drive alternative therapies. The validity of this hypothesis will be explored within the context of acid-base balance in OP, dietary effects of metabolic acidosis (specifically protein and minerals such as potassium (K) and sodium (Na)), and the role of physical activity on pH homeostasis.
ACID-BASE BALANCE IN OSTEOPOROSIS
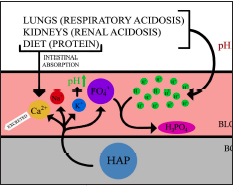
Bone dissolution is a mechanistic phosphate-buffering response to low systemic pH as a result of increased dietary acid load and respiratory and/or renal acidosis (Fig. 1) (Bushinsky 2010). It was first suggested by Wachman and Bernstein (1968) that induced chronic metabolic acidosis and prolonged utilization of the phosphate-buffer system reduces skeletal buffering capacity over time, theoretically explaining age-associated osteoporotic risk. A Western diet high in grain and animal protein has been associated with increased calciuria and net urinary acid production (Jehle 2006, Maurer 2003). This is thought to represent elevated systemic acidity and would contribute towards OP pathogenesis (Jehle 2006).
Figure 1. highlights the outcome of inadequate acid-base buffering in lungs and kidneys contributing to respiratory and renal acidosis, respectively. Although protein increases intestinal absorption of calcium, sulfur-containing amino acids in protein can also contribute towards acidosis. This systemic acid-base imbalance is in part alleviated by the skeletal system. Hydroxyapatite (HAP) typically stored in bone dissociates in response to low pH, releasing Ca, K, magnesium, and phosphate into the circulatory system. The release of phosphate ions neutralizes blood pH by forming H3PO4. Released K ions further alkalinizes systemic pH.
This effect was further substantiated through NH4Cl loading in human subjects (n=14) where bone resorptive Ca loss, demonstrated by acidosis-induced calciuria, occurred in the absence of increased intestinal Ca absorption (Lemann 2003). Furthermore, acidosis has been associated with increased osteoclastic activity in human peripheral blood in vitro and inhibition of osteoblastic bone formation in rats in vitro (Arnett 2007, Brandao-Burch 2005). In a randomized prospective trial of 161 postmenopausal women diagnosed with osteopenia, alkali treatment of 30 mEq/d oral potassium citrate was associated with 1.87%, 1.39%, and 1.98% increased BMD over one year in lumbar spine, femoral neck, and total hip, respectively (Jehle 2006).
PROTEIN
Although the link between metabolic acidosis and bone resorption has been previously established, there is significant debate over which acidogenic influences contribute to OP, as well as the extent of their impacts on systemic pH. Accumulation of acid load has been widely attributed to excessive protein intake and acid buildup via elevated metabolism of sulfur-containing amino acids (methionine and cysteine) found in higher quantities in animal protein (Fenton 2009a, Poupin 2012, Remer 2000). However, the basis of correlations between protein and systemic acidosis relies on the assumption that urinary Ca excretion induced by protein intake is representative of skeletal Ca loss. Instead, a report evaluating acid balance assessment techniques asserted that the quantification of acid balance requires direct evaluation of intestinal absorption and cannot be indirectly assessed through urinary composition (Lemann 2003). Recent theory proposes that the protein-induced calciuric effect may instead be a byproduct of increased intestinal Ca absorption (Bonjour 2009, Levis 2012). It is thought that dietary protein stimulates gastric acid production and increases Ca solubility and bioavailability, thus contributing towards urinary Ca excretion (Kerstetter 2005). Protein causes increased urinary Ca loss, although the source of the excreted Ca is uncertain. These confounding factors have not been recognized until recently.
Population-based, protective effects of protein intake on BMD have been previously observed (Tucker 2001). In the Framingham Osteoporosis Study, dietary habits and BMD measurements of 615 elderly participants were analyzed in a longitudinal cohort study (Tucker 2001). (valium) Animal protein was associated with a stimulating or protective effect on bone mass, and participants with the greatest protein intake had the highest BMD (Tucker 2001). The highest quartile of protein intake consistently showed the lowest BMD loss over four years at the femoral neck and lumbar spine (Tucker 2001). Although study participants were mainly elderly, and one third of subjects had protein intake below the recommended daily allowance; protein was shown to be important in stimulating and maintaining bone growth in older adults (Tucker 2001). Although the mechanism of that effect remained identified, Gaffney-Stomberg et al. (2009) characterized the beneficial effects of protein intake on bone health through mechanisms involving insulin-like growth factor-1 (IGF-1) and parathyroid hormone (PTH) – factors associated with bone growth and resorption, respectively.
In a randomized controlled feeding study of 27 postmenopausal women, high protein intake (20% of daily energy intake) in low-Ca intake individuals (~675 mg/d) significantly increased Ca isotope absorption (29.5% vs. 26.0%) and compensated for the majority of a 0.5 mmol/d increase in calciuria (Hunt 2009). Additionally, in a randomized crossover study comparing (1) low protein and low-potential renal acid load (LPLP) to (2) high protein and high-potential renal acid load (HPHP) diets in 16 postmenopausal women, HPHP diet was associated with increased intestinal Ca absorption (26.5% vs 22.3%, p<0.05) (Cao 2011). Although neither dietary intervention (LPLP and HPHP) was found to influence markers of bone metabolism, upregulation of serum IGF-1, and downregulation of PTH substantiated proposed benefits of protein on bone even after accounting for renal acid load (Cao 2011).
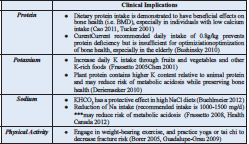
In the context of acid-base balance, it is important to recognize that the compensatory effect of increased intestinal Ca absorption does not completely counterbalance calciuric outcomes (Cao 2011, Hunt 2009). The minimal discrepancy in Ca absorption and excretion may yet contribute towards the etiology of OP through acidosis over time (New 2003). Nonetheless, substantial evidence demonstrating the beneficial effects of protein on bone health, especially in elderly and individuals with low Ca intake, cannot be ignored cannot be ignored. Furthermore, it has been suggested that the current recommended daily intake of 0.8g/kg prevents protein deficiency but is insufficient for optimization of bone health, especially in the elderly (Bushinsky 2010, Gaffney-Stomberg 2009).
POTASSIUM
Aside from high protein intake, the modern Western diet is characterized by energy-dense nutrient-poor foods, including fats, sugars, and Na (Frassetto 2008). It also involves decreased intake of K and HCO3-precursor-rich plants, since the most common plant food ingested is cultivated cereal grain, which yields a net acid load (Sebastian 2002). This diet was only adopted in the last 10 000 years, which is too recent for evolutionary mechanisms to have adjusted in terms of core metabolic machinery (Eaton 1988, Tobian 1988).
Prior to the modern diet, humans ingested a higher ratio of K-to-Na and so the kidneys are programmed to excrete more K than Na (Frassetto 2008). However, this evolutionary mechanism has persisted despite the inversion of the dietary K-to-Na ratio (Eaton 1996). It has been demonstrated that interstitial fluid of bone contains higher concentrations of K and Na than Ca and phosphorus (Krieger 2004). K content is directly related to the amount of consumed and absorbed K and is used by the skeletal system to buffer metabolic acid load (Green 1991, Krieger 2004). Thus, it is important to maintain high levels of K, regardless of food source (Rafferty 2005).
Fruits and vegetables may be dually helpful as they contain both K and HCO3 precursors (Frassetto 2005). It has been demonstrated that in postmenopausal women, higher intake of fruit were positively associated with increased BMD (Chen 2001). Furthermore, increased K content of plant protein relative to animal protein resulted in lowered risk for chronic metabolic acidosis (Deriemaeker 2010).
SODIUM
It has been postulated that high sodium chloride (NaCl) content and low proportion of plant foods in the Western diet induces metabolic acidosis (Frassetto 2008). This effect is compounded by age-related decrease in renal function (Frassetto 2008). It has been suggested that 50-100% of the diet’s net acid load can be attributed to high NaCl intake (Frassetto 2007). Therefore, decreasing the amount of NaCl intake or buffering NaCl with dietary base precursors could help maintain bone mass (Buehlmeier 2012). In a randomized crossover trial, eight male volunteers were randomized into two study campaigns: (1) the experimental group, receiving 90 mmol/d of potassium bicarbonate (KHCO3) to counteract a high NaCl diet (7.3 mmol/kg/d compared to the average NaCl diet of 2.6 mmol/kg/d) and (2) the control group, receiving only a NaCl-rich diet (7.3 mmol/kg/d) (Buehlmeier 2012). It was found that KHCO3 supplementation for ten days decreased NaCl-induced calciuria by 12% (p<0.05), indicating that intake of dietary base precursors may have a protective effect against bone mass loss (Buehlmeier 2012). The authors propose that decreased calciuria is attributed to increased Ca deposition in bone, though these results could be an indication of increased Ca utilization in other body systems(Buehlmeier 2012). Additionally, the adverse effects of NaCl were more persistent than the protective effects of KHCO3 (Buehlmeier 2012). The transient KHCO3 effect is thought to be due to relatively low amounts of KHCO3 (i.e. 90 mmol/d), suggesting that increased levels of KHCO3 may cause a stronger and more protective effect (Buehlmeier 2012).
Considerations of
Data Presented
It has been previously shown that both dietary Ca and urinary Na excretion were significantly correlated with changes in bone mass over a two-year period at the hip and ankle (Devine 1995). Furthermore, the reduction of Na intake has been reported to have beneficial skeletal effects on participants undergoing the Dietary Approaches to Stop Hypertension diet for a month (Lin 2003). In addition, higher dietary Na in young men and women led to increased 1,25-dihydroxyvitamin D and increased intestinal Ca absorption which accounted for Na-induced calciuria (Breslau 1982). It is interesting to note, however, that postmenopausal women did not demonstrate these increased 1,25-dihydroxyvitamin D levels, which may suggest that this population is unable to compensate for the calciuria caused by increased Na ingestion (Breslau 1985). Finally, Frassetto et al. (2008) conclusively demonstrated that dietary NaCl drives urinary Ca excretion, increases bone resorption, and increases the relative rates of bone resorption to bone formation
PHYSICAL ACTIVITY
A lack of research surrounds the effects of physical activity on the body’s acid-base balance. Most research focuses on physical activity as a potential confounder instead of its role in maintaining acid-base homeostasis. Research on physical activity mainly centers on preventative measures rather than therapeutic options for OP (Borer 2005, Guadalupe-Grau 2009). Preventative treatment options include high-resistance physical activity to increase the peak BMD levels in youths, and yoga and tai chi to improve flexibility and reduce fractures among elderly persons (Borer 2005, Guadalupe-Grau 2009). There has been some discussion on the idea that deep breathing associated with yoga and other physical activities could be involved with acid-base balance within the body, as the body regulates acid-base homeostasis through the exhalation of CO2 through the lungs (Horowitz 2009). However, there has not been rigorous research done on this topic, and in order to determine the effects of physical activity on the body’s acid-base homeostasis, further studies need to be conducted.
CONCLUSION
The physiochemical basis for acid-base balance in OP is founded upon sound principles but is not consistently supported by past studies, some of which used inadequate measures of systemic pH (Fenton 2009b, Lemann 2003, Poupin 2012, Remer 2000). Recent studies have found beneficial effects of protein intake on BMD and calcium absorption (Cao 2011, Tucker 2001). Furthermore, HCO3 and K derived from fruit and vegetable metabolism may be promising with regard to net acid load reduction and OP prevention, in addition to other beneficial effects on overall health (Frassetto 2005). However, as contended previously, the Western diet may not be solely responsible for OP pathogenesis since other countries with different dietary patterns exhibit similar patterns in OP prevalence (Fenton 2011). Promising alternative therapies that may aid in the prevention of OP include moderate aerobic exercises, weight-bearing activities, and balance exercises (Borer 2005, Fishman 2009, Guadalupe-Grau 2009, Maciaszek 2007). The clinical implications of findings reviewed in this paper are summarized below (Table 1). Additional etiologic factors may include sunlight exposure, physical labour, and genetic predisposition in these populations (Fenton 2011). Nonetheless, more primary research is needed to fully understand the role of acid-base balance in OP pathogenesis as well as its treatment potential
REFERENCES
Arnett TR, editor. Acid–base regulation of bone metabolism. International Congress Series; 2007: Elsevier.
Bonjour J-P, Chevalley T. The dietary protein-acidosis hypothesis in the pathophysiology of osteoporosis. IBMS BoneKEy. 2009;6(7):254-8.
Borer KT. Physical activity in the prevention and amelioration of osteoporosis in women.Sports Medicine. 2005;35(9):779-830.
Brandao-Burch A, Utting J, Orriss I, Arnett T. Acidosis inhibits bone formation by osteoblasts in vitro by preventing mineralization. Calcified tissue international. 2005;77(3):167-74.
Breslau N, Sakhaee K, Pak C. Impaired adaptation to salt-induced urinary calcium losses in postmenopausal osteoporosis. Transactions of the Association of American Physicians. 1985;98:107.
Breslau NA, McGuire JL, Zerwekh JE, Pak CY.The role of dietary sodium on renal excretion and intestinal absorption of calcium and on vitamin D metabolism.Journal of Clinical Endocrinology & Metabolism. 1982;55(2):369-73.
Buehlmeier J, Frings-Meuthen P, Remer T, Maser-Gluth C, Stehle P, Biolo G, et al. Alkaline Salts to Counteract Bone Resorption and Protein Wasting Induced by High Salt Intake: Results of a Randomized Controlled Trial. Journal of Clinical Endocrinology & Metabolism. 2012;97(12):4789-97.
Bushinsky DA. Acidosis and bone. Nutritional Influences on Bone Health: Springer; 2010. p. 161-6.
Cao JJ, Johnson LK, Hunt JR. A diet high in meat protein and potential renal acid load increases fractional calcium absorption and urinary calcium excretion without affecting markers of bone resorption or formation in postmenopausal women. The Journal of nutrition. 2011;141(3):391-7.
Chen Y, Ho S, Lee R, Lam S, Woo J. Fruit intake is associated with better bone mass among Hong Kong Chinese early postmenopausal women. J Bone Miner Res. 2001;16(suppl 1):S386.
Deriemaeker P, Aerenhouts D, Hebbelinck M, Clarys P. Nutrient Based Estimation of Acid-Base Balance in Vegetarians and Non-vegetarians. Plant foods for human nutrition. 2010;65(1):77-82.
Devine A, Criddle RA, Dick IM, Kerr DA, Prince RL. A longitudinal study of the effect of sodium and calcium intakes on regional bone density in postmenopausal women.The American journal of clinical nutrition. 1995;62(4):740-5.
Duque G, Kiel DP. Osteoporosis in Older Persons: Pathophysiology and Therapeutic Approach: Springer; 2008.
Eaton SB, Eaton SB, Konner MJ, Shostak M. An evolutionary perspective enhances understanding of human nutritional requirements. The Journal of nutrition. 1996;126(6):1732-40.
Eaton SB, Konner M, Shostak M. Stone agers in the fast lane: chronic degenerative diseases in evolutionary perspective. The American journal of medicine. 1988;84(4):739-49.
FAO W. Vitamin and mineral requirements in human nutrition, Geneva.World Health Organization. 2004.
Fenton TR, Lyon AW. Milk and acid-base balance: proposed hypothesis versus scientific evidence. Journal of the American College of Nutrition. 2011;30(5 Supplement 1):471S-5S.
Fenton TR, Lyon AW, Eliasziw M, Tough SC, Hanley DA.Meta‐Analysis of the Effect of the Acid‐Ash Hypothesis of Osteoporosis on Calcium Balance.Journal of Bone and Mineral Research. 2009;24(11):1835-40.
Fenton TR, Lyon AW, Eliasziw M, Tough SC, Hanley DA. Phosphate decreases urine calcium and increases calcium balance: a meta-analysis of the osteoporosis acid-ash diet hypothesis. Nutr J. 2009;8:41.
Fishman LM. Yoga for osteoporosis: A pilot study. Topics in Geriatric Rehabilitation. 2009;25(3):244-50.
Foundation NO.Clinician’s guide to prevention and treatment of osteoporosis.National Osteoporosis Foundation Washington DC; 2010.
Frassetto L, Morris RC, Sebastian A. Long-term persistence of the urine calcium-lowering effect of potassium bicarbonate in postmenopausal women. Journal of Clinical Endocrinology & Metabolism. 2005;90(2):831-4.
Frassetto LA, Morris RC, Sebastian A. Dietary sodium chloride intake independently predicts the degree of hyperchloremic metabolic acidosis in healthy humans consuming a net acid-producing diet. American Journal of Physiology-Renal Physiology. 2007;293(2):F521-F5.
Frassetto LA, Morris RC, Sellmeyer DE, Sebastian A. Adverse effects of sodium chloride on bone in the aging human population resulting from habitual consumption of typical American diets. The Journal of nutrition. 2008;138(2):419S-22S.
Gaffney-Stomberg E, Insogna KL, Rodriguez NR, Kerstetter JE. Increasing dietary protein requirements in elderly people for optical muscle and bone health. Journal of the American Geriatrics Society. 2009;57:1073-9.
Garriguet D. Bone health: Osteoporosis, calcium and vitamin D. In: Canada S, editor. Health Reports 2011.
Guadalupe-Grau A, Fuentes T, Guerra B, Calbet JA. Exercise and bone mass in adults. Sports Medicine. 2009;39(6):439-68.
Horowitz S. Acid–Base Balance, Health, and Diet.Alternative and Complimentary Therapies. 2009;15(6):292-7.
Health Canada. (June 8, 2012). Sodium in Canada. In Health Canada – Food and Nutrition. Retrieved April 1, 2013, from http://www.hc-sc.gc.ca/fn-an/nutrition/sodium/index-eng.php.
Hunt JR, Johnson LK, Roughead ZF. Dietary protein and calcium interact to influence calcium retention: a controlled feeding study. The American journal of clinical nutrition. 2009;89(5):1357- 65.
Jehle S, Zanetti A, Muser J, Hulter HN, Krapf R. Partial neutralization of the acidogenic Western diet with potassium citrate increases bone mass in postmenopausal women with osteopenia.Journal of the American Society of Nephrology. 2006;17(11):3213-22.
Kanis J, Odén A, Johnell O, Johansson H, De Laet C, Brown J, et al. The use of clinical risk factors enhances the performance of BMD in the prediction of hip and osteoporotic fractures in men and women. Osteoporosis International. 2007;18(8):1033-46.
Kerstetter JE, O’Brien KO, Caseria DM, Wall DE, Insogna KL.The impact of dietary protein on calcium absorption and kinetic measures of bone turnover in women.Journal of Clinical Endocrinology & Metabolism. 2005;90(1):26-31.
Krieger NS, Frick KK, Bushinsky DA.Mechanism of acid-induced bone resorption.Current opinion in nephrology and hypertension. 2004;13(4):423-36.
Lemann J, Bushinsky DA, Hamm LL. Bone buffering of acid and base in humans.American Journal of Physiology-Renal Physiology. 2003;285(5):F811-F32.
Levis S, Lagari VS. The Role of Diet in Osteoporosis Prevention and Management.Current osteoporosis reports. 2012;10(4):296- 302.
Lin P-H, Ginty F, Appel LJ, Aickin M, Bohannon A, Garnero P, et al. The DASH diet and sodium reduction improve markers of bone turnover and calcium metabolism in adults. The Journal of nutrition. 2003;133(10):3130-6.
Maciaszek J, Osiński W, Szeklicki R, Stemplewski R. Effect of Tai Chi on body balance: randomized controlled trial in men with osteopenia or osteoporosis. The American journal of Chinese medicine. 2007;35(01):1-9.
Maurer M, Riesen W, Muser J, Hulter HN, Krapf R. Neutralization of Western diet inhibits bone resorption independently of K intake and reduces cortisol secretion in humans. American Journal of Physiology-Renal Physiology. 2003;284(1):F32-F40.
Nase JB, Suzuki JB. Osteonecrosis of the jaw and oral bisphosphonate treatment. J Am Dent Assoc. 2006;137(8):1115- 9.
New SA. Intake of fruit and vegetables: Implications for bone health. Proceedings of the Nutrition Society. 2003; 52:889-99.
Papaioannou A, Morin S, Cheung AM, Atkinson S, Brown JP, Feldman S, et al. 2010 clinical practice guidelines for the diagnosis and management of osteoporosis in Canada: summary. Canadian Medical Association Journal. 2010;182(17):1864-73.
Poliquin S, Joseph L, Gray-Donald K. Calcium and vitamin D intakes in an adult Canadian population.Canadian Journal of Dietetic Practice and Research. 2009;70(1):21-7.
Poupin N, Calvez J, Lassale C, Chesneau C, Tomé D. Impact of the diet on net endogenous acid production and acid–base balance. Clinical Nutrition. 2012;31(3):313-21.
Rachner TD, Khosla S, Hofbauer LC. Osteoporosis: now and the future. The Lancet. 2011;377(9773):1276-87.
Rafferty K, Davies KM, Heaney RP. Potassium intake and the calcium economy.Journal of the American College of Nutrition. 2005;24(2):99-106.
Remer T, editor. ACID‐BASE IN RENAL FAILURE: Influence of Diet on Acid‐Base Balance. Seminars in Dialysis; 2000: Wiley Online Library.
Sebastian A, Frassetto LA, Sellmeyer DE, Merriam RL, Morris RC. Estimation of the net acid load of the diet of ancestral preagricultural Homo sapiens and their hominid ancestors.The American journal of clinical nutrition. 2002;76(6):1308-16.
Tarride J-E, Hopkins R, Leslie W, Morin S, Adachi J, Papaioannou A, et al. The burden of illness of osteoporosis in Canada.Osteoporosis International. 2012;23(11):2591-600.
Tobian L.The Volhard lecture.Potassium and sodium in hypertension. Journal of hypertension Supplement: official journal of the International Society of Hypertension. 1988;6(4):S12.
Tucker KL, Hannan MT, Kiel DP. The acid-base hypothesis: diet and bone in the Framingham Osteoporosis Study. European journal of nutrition. 2001;40(5):231-7.
Wachman A, Bernstein DS. Diet and osteoporosis.The Lancet. 1968;291(7549):958-9.
Farid Wassef

Integrated Medicine is the Key to Success
Farid Wassef is not your typical pharmacist. Here’s a look at how he developed his store and practice and why he’s now running for office to try to make positive changes to the health care system.
By: Nancy Ripton
Photography: John Milios
“When you act in the interest of the patient – and put their interest before your own – you provide optimal health care,” says Farid Wassef. It was this thinking that encouraged Wassef to open a clinic adjacent to his Stouffville, Ontario pharmacy practice 20 years ago. In fact, Wassef has always felt that integrated medicine is in the best interest of everyone involved in health care.
Born into Pharmacy
Wassef is a second-generation pharmacist who has worked and lived in Stouffville, Ontario for over 40 years. The family pharmacy was first owned by Wassef’s father Lou Wassef who purchased the pharmacy in 1974 after emigrating from Egypt in 1968 when Farid was just four years old.
Growing up, Wassef helped out in the family pharmacy and saw at an early age the need for alternative forms of health care. “Even then I could see the effect the environment, stress, diet, lack of exercise – so many things – were contributing to people getting chronic illness. They just weren’t being addressed,” says Wassef.
After graduation from the Massachusetts College of Pharmacy in 1989, Wassef took over management of the family pharmacy and his disillusionment with traditional medicine continued to grow.
“The pharmacist typically has two or three minutes to spend with a patient when they are giving them their prescription,” says Wassef. “I became very frustrated with this model that only allows a couple of minutes to interact with a patient at the pharmacy counter.” Wassef felt he had more to share than that amount of time could afford.
Changing the Definition of Pharmacist
In 1993, Wassef decided to set up a clinical practice to support his pharmacy. “When I started there was a very narrow view that people got sick because of genetics,” says Wassef. “I took a lot of pain and inflammation syndromes that went un- or over-treated with medications and helped patients understand that they had other options.”
His patient consultation practice involved integrating lifestyle changes, nutrition, and natural health products with pharmaceutical care. “Within the scope of the practice of pharmacy, a pharmacist is permitted to counsel on prevention and treatment of disease, counsel on diet, lifestyle, nutritional and nutraceutical supplements, botanical medicines, and – of course – pharmaceutical drugs,” says Wassef. “While a pharmacist may not be permitted the act of diagnosis, I found many MD’s in the Stouffville and the surrounding area were eager to collaborate with an objective and evidence-based person providing good information on natural medicines. Through these collaborations we were able to offer patients a broad array of integrative diagnostic techniques in addition to standard laboratory procedures.”
Of course, it wasn’t easy finding doctors to collaborate with at first. “People started singing praises to their physicians,” says Wassef. “People were getting better and it was a threat to physicians at first until they realized we could work together.”
The idea of a pharmacist talking about alternatives to prescriptions may at first seem counterintuitive but in addition to being best for the patients it is also a great business decision.
“Pharmaceutical companies realized that they can’t over market to the point where their product becomes misused and is taken off market,” says Wassef. “They want to make sure the drugs are taken appropriately.” The discontinuation rates for most drugs are high after six months. If you give less medication (to people who are healthier and eating right) they are more likely to stay on it for longer and have better results.
“There is a pharmaceutical shift to promoting exercise, diet and fish oil,” says Wassef. Even Pfizer now owns Emergen-C. The pharmaceutical companies are becoming integrated and more patient centered and focused on health.
Wassef’s father (who passed away in 2004) was supportive of his son from the beginning. “Coming from Egypt the idea of alternative medicine wasn’t foreign to him,” says Wassef. “He would compound Echinacea and ginseng in 50s and 60s.” He adds that “Ultimately, it’s about good medicine and good outcomes for the patient.
Extending His Reach
Wassef was not satisfied with his role as pharmacist and practitioner. He was driven to spread the word to other pharmacists, doctors and anyone else who would listen as to the power of diet and lifestyle in health promotion, disease prevention and disease treatment. He was also eager to educate his fellow pharmacists as to the role they could and should be playing in their patients’ care.
Working with the Institute of Functional Medicine (whom Wassef credits with providing most of the training he relies upon as a practitioner of integrative medicine), Wassef created a continuing education curriculum for pharmacists to receive training in integrative medicine. He also lectures across North America to pharmacists and doctors regarding application of integrative medicine, and methods through which integrative minded pharmacists can successfully collaborate with MD’s in their community. His immense efforts to move the discipline of integrative medicine forward earned him the 2006 award for Canadian Pharmacist of the Year.
While juggling the roles of a pharmacy manager, seeing 80-plus patients per week, authoring over 200 articles, CE courses, and books (including Breaking the Age Barrier – Strategies for Optimal Health, Longevity, and Energy published by Penguin in 2003), and his ongoing industry consulting and speaking engagements, yet another intriguing path caught Wassef’s eye – politics.
The idea of impacting healthcare from a “top down” approach made a lot of sense to Wassef. “I’ve been a strong advocate for my profession for last 20 years,” he says. “I got tired of hearing I had lovely ideas, but there’s no money. There is money! It’s just being wasted. Our current health care system is not in the best interest of the public.”
Wassef slowly molded his career to be able to take on the workload politics would entail. He sold ownership of his pharmacy and merged with the local IDA team, where he maintains an office and his practice to this day. He cut back on time with patients, yet maintains an important practice within the Stouffville IDA pharmacy, and continues to welcome public speaking arrangements.
It was 2009 when Wassef first actively participated in a political role, attempting to block proposed cuts to the healthcare system (that subsequently came into effect in 2010). The final straw that brought Wassef to action was the interpretation that the $1.2 billion e-health scandal is what necessitated healthcare cuts in the first place. (They’ve now spent two billion.)
The PC party of Ontario approached Wassef in 2010 after witnessing his passion and determination to change the system. In 2011 he secured his nomination as the PC candidate for the riding of Stouffville, Markham, Richmond Hill, and King townships. He lost the 2011 election to the incumbent Liberal candidate, but Wassef has been re-nominated and will stand in the next general election as the PC Candidate for Oak Ridges-Markham for Member of Provincial Parliament.
Wassef is determined to improve our healthcare system, which he believes should focus more on disease prevention and extending an individual’s functional health. He wants the money to go where it can be most effective. To move the system more towards preventative care and to stop over- and mis-appropriate prescriptions. Now that’s something we can all cast our vote for.
Pull quotes:
The practice of integrative medicine begins, grows, and thrives through one common seed – passion. Passion to help others, to solve mysteries commonplace answers simply don’t make sense for and, ultimately, to achieve maximum positive impact for people using the least invasive strategy available.
Weight loss, prevention of cold and flu, arthritis and sleep issues are the four most common complaints Wassef hears. Natural alternatives can help with all of them.





