





A new articulation agreement between the Canadian Memorial Chiropractic College (CMCC) and the University of Ontario Institute of Technology (UOIT) will enable qualified students to complete a Bachelor of Health Sciences (Honours) in Kinesiology degree and a Doctor of Chiropractic degree in seven years, instead of eight. For individuals who identify their career path early, this agreement seamlessly bridges a foundational degree into a professional degree in chiropractic. “UOIT and CMCC share a commitment to innovation in education,” said UOIT President Tim McTiernan, PhD. “This accelerated pathway will enable our students to further their education in less time so they can take an active role in helping others. In addition, cross appointments between our two institutions will enable the sharing of expertise and knowledge resources, allowing us to fully leverage the academic excellence resident at both institutions.” Acceptance into the CMCC-UOIT Bridging Program will begin in September 2012.
Harper government invests in personalized medicine
The Harper Government announced an important investment that will help Canadians receive more effective treatments and make the healthcare system more sustainable through personalized medicine. Healthcare will evolve from a reactive “one-size-fits-all” system towards a system of predictive, preventive, and precision care. Areas in which personalized approaches are particularly promising include oncology, cardiovascular diseases, neurodegenerative diseases, psychiatric disorders, diabetes and obesity, arthritis, pain, and Alzheimer’s disease. In all of these fields, and others, a personalized molecular medicine approach is expected to lead to better health outcomes, improved treatments, and reduction in toxicity due to variable or adverse drug responses. In addition to saving on the costs of expensive drug treatments, this personalized treatment would prevent a great deal of suffering, while identifying and initiating earlier treatments that would be more effective.animal data indicates AFN-1252 has mg/ kg efficacy that is significantly improved compared to linezolid; and both single and multiple dose Phase 1 data indicate an excellent safety and tolerability profile. We are confident that the Phase 2 trial will confirm AFN-1252 as a potent and well tolerated anti-Staph antibiotic” commented Dr. Hafkin, Chief Medical Officer of Affinium Pharmaceuticals.
Northern Centrefor Integrative Medicine

Rural ND’s embrace role of community primary care provider
Cher Boomhower, ND and Jason Boxtart, ND founded the Northern Centre for Integrative Medicine a decade ago with a vision of delivering top quality healthcare to one of Canada’s many under-serviced rural areas; Prince George, British Columbia. Naturopathic doctors often find the practice management challenges of starting a new practice difficult, and thus the husband and wife team are quick to showcase the need for good quality healthcare in rural settings. “A lot of people in rural settings do not have a family physician, and as a result we enjoyed very rapid practice growth”, describes Jason. “More new grads should seek out opportunities in rural settings… we have found conventional physicians practicing in rural settings to be much more open to integrative practices, if for no other reason out of a need for help in managing the healthcare needs of the community! And with the arrival of broad prescription rights in British Columbia, our role as an important, first-line primary healthcare provider has been solidified”.

Cher and Jason go on to describe several keys to the success the facility enjoys today. Chief among them was the conscious decision to establish what the team describes as “portals of entry” into the practice. By establishing a broad array of distinct services, patients initially arriving to have a particular concern addressed quickly become patients of the facility as a whole. Initially arriving for help with pain, patients are eager to then enter the weight loss program, investigate their body burden of environmental contaminants, or perhaps seek entry into the preconception/ fertility program.

The duo has remained true to their professions oath in terms of endless continuing education and training, making possible the immensely broad and diverse array of services offered at the facility. The two ND’s have also selected different avenues of further training along the way, making each an “expert” in quite differing applications of naturopathic medicine. Jason is currently working towards completion of the Fellowship of the American Board of Naturopathic Oncology (FABNO) and the American Association of Anti Aging Medicine (AAAAM) designations, and has completed training in prolotherapy and mesotherapy. Therefore, his areas of specialization in the facility, and thus the programs of the clinic under his direction include cancer management, pain management, weight loss, and health and beauty. Cher completed Dr Crinnion’s three year extended program in environmental medicine, training in integrative approaches for mental health concerns, and expertise in the delivery of colon hydrotherapy. As such, Cher manages programs within the facility that include environmental medicine, mental health, chelation, fertility and preconception, and IV nutrient therapies.
A carefully selected team of associates further expanded the impressive list of services. Sonya Redden is a physiotherapist that has been with the team since the opening of the facility. In addition to conventional physiotherapy services, Sonya has made manual lymphatic drainage an available service. Heidi Kaseweter is a certified counselor who has proven invaluable to the team, responsible for much of the success of the weight management program and mental health program of the facility. Jane Hedges is a registered midwife that joined the team approximately three years ago. She provides an ideal fit for the growing preconception/ fertility program.

The Northern Centre for Integrative Medicine has also enjoyed the recent collaboration of Dr Shona Imlah, MD. Shona is a family physician with an expertise in OBGYN. Shona works with the team two days a week, with Cher and Jason hoping she will expand her role moving forward. Among the multitude of services Shona offers, her arrival has established the bioidentical hormone therapy program of the facility.

Cher and Jason showcase the many diverse ways naturopathic doctors are able to impact the healthcare landscape of our country. First and foremost a naturopathic doctor is called upon to deliver their safe and effective system of care to the public, and the team sets an impressive standard in this regard. The Northern Centre for Integrative Medicine boasts over 200 patient visits per week. Beyond practice the team has entrenched themselves in roles that are shaping both the naturopathic and conventional medical fields.
For the past eight years Cher and Jason have served as adjunct faculty for the University of British Columbia (UBC) and the University of Northern British Columbia (UNBC). They help deliver a UNBC course in their school of medicine; “Doctor, Patient, and Society”. How the course came about is an interesting story; the Dean of the program was brought in from Scotland and was displeased with the lack of training students were receiving in integrative medicine. Cher and Jason do not deliver a curriculum of naturopathic theraputics, but the Dean realized interaction with two evidence- based ND’s would in-and-of-itself deliver valuable knowledge in the realm of integrative medicine to students. Cher and Jason describe a transformation over the years of students first seeming to not care of anything non- pharmaceutical, to today’s students eager to learn anything they can of application of nonconventional practices. To further deliver knowledge of integrative medicine to aspiring MD’s, Cher and Jason’s private clinic is an optional site for students to conduct a two to four week rotation during their third year.
Jason further places naturopathic medicine in the limelight in a number of ways. He has been the Chair of the Canadian Association of Naturopathic Doctors for the past three years, serving as a board member for two years previous. He thus played an important role in witnessing British Columbia securing broad scope of practice and prescription privileges, and likewise helps the process in Ontario, although Ontario does not appear destined for the good fortune our friends to the west achieved.

Jason’s enrollment in the FABNO designation has lead to some impressive aspirations. Jason is in talks with Dr Hal Gunn and the team of Inspire Health to create satellite clinics of the incredibly successful Vancouver model of the concept. Dr Gunn won the Rogers Prize for establishing a truly integrative model of cancer care. We wish Jason much success in creating such a landmark facility. Also, we hope Cher and Jason would then consider serving as a site to accept residents for FABNO training of newly graduated ND’s, relieving some of the burden of the residency program currently principally managed by the Cancer Treatment Centres of America.

I do not think Cher and Jason envisioned their current position when they opened their doors to the Prince George community a decade ago. First came a dedication to provide excellent care. As is typically the case, the rest snowballs from there. Today they exemplify a quality facility of integrative medicine, while devoting tremendous resources of time to improve the political landscape of the profession moving forward. Reaching aspiring MD’s one at a time through education, reaching politicians through appointment to the Chair of our national association, and aspiring to expand the most recognized integrative cancer facility in the country are a handful of ways Cher and Jason have found to give to the profession as they have given to their community since their opening day.
Vyana Wellness Naturopathic Clinic

Vyana is a Sanskrit word meaning an expanding life force or breath. Since breath is essential for health and Maya Jobanputra, ND, believes that health can be restored by addressing basic, core concepts, this term seemed appropriate to represent her vision of a multidisciplinary clinic. Vyana Wellness, located in Waterloo, Ontario, opened in 2009 and currently over 150 patients walk through its doors on a weekly basis. Maya’s intention of opening a clinic was to create a safe, inviting, and healing environment where patients can feel at home. She wanted this feeling of comfort to extend to the practitioners of Vyana as well so that all staff could share the space and utilize it as their own in an effort to foster positivity, growth, and creativity. She notes that too often health clinics build their business models around the owner, often to the neglect of individual practitioners. Therefore, Vyana’s goal is to provide a sense of community not only for patients, but also staff.


To meet the specific and varied needs of the public while successfully cultivating a community feeling, Vyana felt that it was necessary to provide a wide array of services, including naturopathic medicine, chiropractic, osteopathic manipulative therapy, acupuncture, massage therapy, counseling, reiki, bodytalk, bowen therapy, and life coaching. The team of Vyana Wellness that delivers these diverse services is comprised of a clinic administrator and eight practitioners.
The facility is 1600 square feet of utilized floor space with six treatment rooms. Unique to Vyana is a large multipurpose room measuring roughly 275 square feet that is used for yoga classes. These classes are offered for a minimal fee to increase the scope of offerings available to the public. This space is also used to host free workshops open to the public. Collaboration among practitioners to deliver these educational sessions is encouraged since Vyana strongly believes that health and illness are multi-dimensional. It is also within this multipurpose room that Vyana hosts “Fix-it” days where the clinic doors are opened to the public on designated weekends. All practitioners are available to offer free consultations for anyone who would like to learn how to optimize health. Thus far, these “Fix-it” days have proven very successful. Vyana plans to expand the use of its versatile multipurpose room in an effort to strengthen the sense of community within the clinic. Long-term goals are to offer a full yoga schedule, relaxation classes, support groups, and a broadened scope of seminars and trainings. Vyana is also in possession of an additional 1600 square feet of space that can be utilized as expansion occurs.

The facility boasts a diverse dispensary, offering products from such companies as Ascenta, Genestra, Metagenics, Bioclinic, Mediherb, and Pascoe and there are plans to expand in the near future. Vyana also provides natural and non-toxic personal health products, such as body wash, shampoo, and conditioners since quality skin care is an important component of a healthy lifestyle. A number of integrative tests are made available to patients, the most popular being IgG food sensitivity, salivary hormone, and various blood panels (i.e., thyroid, complete blood count, etc).

Vyana focuses marketing efforts online. Google AdWords offers pay-per-click advertising with local distribution. When people search on Google using one of Vyana’s designated keywords, their ad appears next to the search results. The clinic also regularly updates its website with news, recipes, and YouTube videos while providing links to its monthly newsletters. In line with the goal of creating a community feeling, Vyana is working to create an online community through regular Facebook and Twitter updates. The clinic is finding that these social media are providing a good solid foundation for a thriving online community. In fact, Vyana has found that about half of the new patients coming through its doors are coming from internet marketing and half are coming from referrals. Each practitioner provides input with these marketing methods as equality of services is a key concept highlighted at Vyana.

IHP is grateful to the team at Vyana Wellness for allowing us to profile their clinic. Although the clinic has only been in operation for a little more than two years, it is quickly establishing an excellent reputation. While nurturing and encouraging their increasing community, we expect many successes for this eclectic group of practitioners.
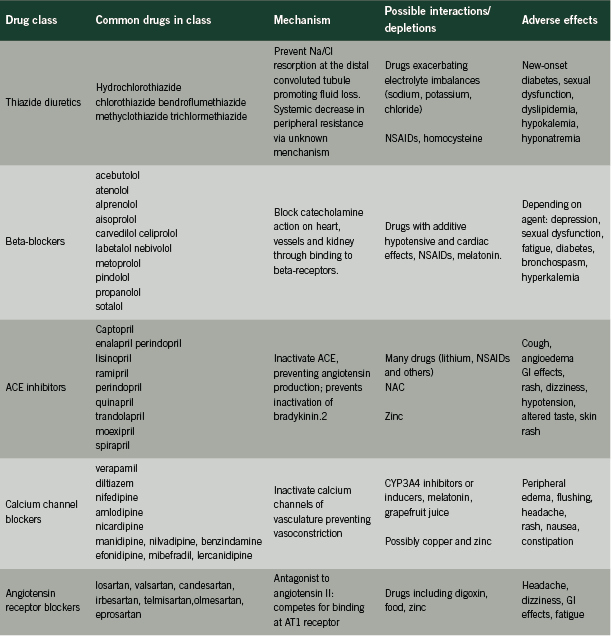
First- line antihypertensives

First- line antihypertensives
Mechanisms of action, adverse effects and potential interactions
Hypertension is estimated to affect 23% of the Canadian population, or approximately six million adults. Prevalence increases with age: more than 70% of adults over the age of 80 are affected by this condition (Robitaille 2011).
Elevated blood pressure is a well-established risk factor for cardiovascular events including myocardial infarction and stroke (Leone 2011). Chronic kidney disease and other conditions are complicated and exacerbated by hypertension (Koizumi 2011). In light of the risks associated with this presentation, blood pressure reduction is an important therapeutic goal.
Although lifestyle changes including weight reduction, exercise prescriptions and diet modifications are primary recommendations in sustainable hypertension management, pharmacological therapies are commonly used. Current recommendations from the Canadian Hypertension Education Program (CHEP) indicate that first-line drug therapy should consist of one of the following agents:
• A thiazide diuretic;
• A beta-blocker;
• An angiotensin-converting enzyme inhibitor (ACE inhibitors);
• A long-acting calcium channel blocker (CCB); or
• An angiotensin receptor blocker (ARB). Should monotherapy be ineffective, a combination of select agents is encouraged (Rabi 2011).
This review will examine these five classes of drugs, describing their mechanism of action, adverse effects and potential interactions with drugs, nutrients and endogenous substances.
Mechanisms of blood pressure regulation
Adequate circulatory pressure ensures appropriate perfusion of all tissues of the body, supporting the delivery of oxygen, nutrients and other essential factors to all cells. The crucial task of blood pressure regulation relies upon the interplay of numerous physiologic systems.
The renin-angiotensin-aldosterone system (RAAS) is integral to the dynamics of blood pressure regulation (Crowley 2007) and has a powerful influence upon vascular tone and fluid volume. This system is the target of ACE inhibitors and ARBs.
Renin, a proteolytic enzyme, is central to the RAAS. Once secreted by the juxtaglomerular cells of the kidneys, renin cleaves inactive angiotensinogen circulating in the blood. Angiotensin I is formed and converted in turn to angiotensin II by angiotensin-converting enzyme (ACE) (Raebel 2011). Angiotensin II goes on to stimulate angiotensin 1 receptors (AT1) in the heart, blood vessels, kidney, adrenals and brain, causing vasoconstriction, vasopressin and aldosterone release, sodium retention and increased sympathetic activity (Burnier 2001, Raebel 2011). Systemic blood volume and pressure increase as a result.
Interactions between ACE and bradykinin further increase circulatory pressure. Bradykinin promotes vasodilation through nitric oxide release while encouraging salt loss through the urine (Piepho 2000); ACE inactivates bradykinin through a cleaving process.
Calcium dynamics are important to the maintenance of vascular tone (Richard 2005). Influx of calcium across cell membranes causes contraction of smooth muscle cells lining the circulatory system, resulting in vasoconstriction and an increase in blood pressure. This mechanism is the therapeutic target of calcium channel blockers (CCBs).
The sympathetic nervous system can induce changes in vascular tone, renin levels and cardiac function. Adrenergic receptors in numerous organs and tissues respond to catecholamine release causing:
• increased heart rate and output (through beta-1 receptors);
• vasoconstriction and vasodilation (through alpha-2 and beta-2 receptors); and
• increased renin production (through beta-1 receptors).
Beta-type adrenoreceptor blocking drugs (beta-blockers) act upon these receptors with varying degrees of selectivity (Gorre 2010).
Finally, appropriate blood pressure levels require adequate intravascular fluid. Complex neurohormonal mechanisms involving the kidneys, the thirst response, aldosterone and anti-diuretic hormone (ADH) ensure that fluid is conserved and excreted from the body as needed (Thornton 2010).Thiazide diuretics influence this system, promoting fluid loss and decreasing blood pressure.
THIAZIDE DIURETICS
Thiazide diurectics have been used in the management of hypertension for over 50 years (Sarafidis 2010). Still considered a first-line agent, thiazide diuretics appear to be more beneficial than other anti-hypertensives in their ability to reduce cardiovascular morbidity and mortality (Wright 2009). Thiazide diuretics have also been shown to be more effective than ACE inhibitors or ARBs in patients of African descent (Taylor 2005).
Mechanism of action
Thiazide diuretics act at the distal convoluted tubule of the nephron, inhibiting the activity of the NaCl co-transport pathway (Sarafidis 2010). The action of these drugs prevents the resorption of sodium and chloride at this site and promotes fluid loss through the urine.
Paradoxically, fluid levels return to pre-treatment levels within four to six weeks of treatment initiation, yet pressure decrease is maintained. This hypotensive effect may be explained through the apparent ability of thiazide diuretics to reduce peripheral vascular resistance and blood pressure, but the mechanism is not understood at present (Duarte 2010).
Adverse effects
Higher levels of sodium in the collecting duct of the nephron result in increased potassium loss, creating the potential for both hyponatremia (Egom 2011) and hypokalemia. Potassium loss can increase the risk of sudden cardiac death although the use of lower-dose regimens and concurrent ACE inhibitors may attenuate this risk (Krämer 2000). Hypokalemia is cited as a possible cause of new-onset diabetes associated with thiazide diuretic use (Sica 2011). Magnesium loss (Sarafidis 2010) and uric acid retention (Sica 2011) are also associated with thiazide diuretic use.
Erectile dysfunction has been reported in men using thiazide diuretics (Francis 2007). Dyslipidemia has also been attributed to thiazide use, but newer research suggests inconsistent effects upon lipid levels in the absence of increased cardiovascular risk (Deano 2012).
Potential interactions
Care should be taken with any drugs that decrease potassium, magnesium or sodium levels as an additive effect may result. The hypotensive effect of thiazide diuretics may be decreased with NSAID use (Sica 2011). Digoxin intoxication has been associated with concomitant diuretic use (Wang 2010).
Plasma homocysteine levels may be increased with thiazide diuretic use (Westphal 2003). Additional monitoring of homocysteine levels may be necessary in these patients.
BETA-BLOCKERS
Beta-blockers have been used since the mid-1960’s in the management of cardiovascular conditions (Chrysant 2008). This diverse class includes both lipophilic and hydrophilic drugs, varying in their receptor selectivity and duration of effect. Beta-blockers continue to be considered first line agents in the management of hypertension (Rabi 2011) despite recent criticisms of their ability to prevent stroke and other negative outcomes in comparison to other anti-hypertensives (Wiysonge 2007).
Mechanism of action
Beta-blockers exert their influence by competing with catecholamines for absorption by beta-1 adrenergic receptors. This binding blocks the effect of endogenous neurotransmitters, decreasing the effects of the sympathetic nervous system causing reduced blood pressure, heart rate and cardiac contractility. Non-selective beta-blockers such as propanolol may also act upon beta-2 receptors in the lungs, causing undesirable pulmonary effects in some individuals (van der Woude 2005). Newer agents (carvedilol and nebivolol) promote additional vasodilation through nitric oxide production (Chrysant 2008).
Adverse effects
Depression associated with beta-blocker prescription has been reported in the literature (Patten 1990) although much current research does not support this association (Ko 2002, Verbeek 2011). Others suggest that while depressive symptoms may occur with beta-blockers use, the effect is limited to lipophilic agents (propanolol, alprenolol) that can cross the blood-brain barrier (Luijendijk 2011).
Sexual dysfunction and fatigue have been associated with beta-blocker use (Ko 2002) but may again be related to the specific agents used (Brixius 2007). In addition, some beta-blockers may increase the risk of developing new-onset diabetes (Gorre 2010). It is unclear whether newer vasodilating agents such as carvedilol, nebivolol and labetolol share these properties with older agents (Ram 2010).
Non-selective beta-blockers have been contraindicated in patients with lung disorders as inhibition of the beta-2 adrenoreceptors in the lungs may cause bronchospasms in these patients (Kendall 1997). Newer drugs that are selective for beta-1 receptors have not been found to cause the same issues and appear to be safe for use in patients with pulmonary concerns (Salpeter 2005).
Like ACE inhibitors and ARBs discussed below, beta-blockers increase the risk of hyperkalemia as a result of decreased renin production (Takaichi 2007).
Potential interactions
Care should be taken with concomitant use of any other drugs with hypotensive or negative inotropic or chronotropic effects. Interactions between beta-blockers and NSAIDs such as ibuprofen have also been reported in the literature (Salort- Llorca 2008) resulting in decreased effectiveness of this antihypertensive medication.
Melatonin production appears to be impaired by some beta-blockers (Stoschitzky 1999) with the notable exception of carvedilol. Melatonin supplementation may be indicated in patients treated with drugs from this class (Fares 2011).
ACE INHIBITORS
ACE inhibitors form a diverse group of drugs that inhibit the RAAS through their action upon angiotensin-converting enzyme (ACE).
Mechanism of action
ACE inhibitors bind to ACE through the formation of zinc ligands (Piepho 2000). The production of angiotensin II is thereby impaired, preventing AT1-mediated increases in vascular tone, aldosterone production and bradykinin degradation (Hayduk 1999). The RAAS is essentially inactivated, preventing further increases in blood pressure.
Adverse effects
The most common adverse effect associated with ACE inhibitor use is a dry cough (Semple 1995) that while not serious, can prompt treatment discontinuation. Cough is believed to be associated with an accumulation of bradykinin secondary to ACE inhibition (Mas 2011).
Patients using ACE inhibitors are also at risk of hyperkalemia (Raebel 2011), resulting from the ACE-mediated decrease in aldosterone production (Piepho 2000). This adverse effect may be more pronounced with concomitant renal or cardiac failure (Izzo 2011). ACE inhibitors are not recommended in patients with renal stenosis (Parish 1992). Other reported adverse effects include angioedema (Izzo 2011), rash, dizziness, gastrointestinal (GI) effects, hypotension and altered taste (Parish 1992).
The safety of ACE inhibitors has not been clearly established in pregnancy. Although significant adverse effects to the fetus have not been seen in some trials (Diav-Citrin 2011), this class of drugs is generally regarded as contraindicated during pregnancy (Cooper 2006, Izzo 2011).
Potential interactions
Many drug-drug interactions are possible with ACE inhibitor use (Hines 2011). Lithium toxicity is possible with concurrent ACE inhibitor use (Piepho 2000) and NSAIDs can decrease the anticipated hypotensive effect of this intervention (Piepho 2000, Salort-Llorca 2008).
A small crossover study found that N-acetyl cysteine (NAC) may potentiate the hypotensive effect of captopril and enalapril (Barrios 2002). This may be a desirable effect in some patients. Endogenous zinc levels may be depleted by ACE inhibitor use (Golik 1998)
CALCIUM-CHANNEL BLOCKERS (CCBs)
CCBs have been in use for half a century (Nayler 1986) and have evolved through several generations of drugs from short-acting drugs (verapamil), through longer-acting drugs (nisoldipine), to newer, slower-release drugs with great affinity for their designated receptors (manidipine, lercanidipine) (Richard 2005).
Mechanism of action
Contraction of muscular tissue lining the circulatory system is mediated in part by intracellular calcium levels. CCB-type drugs bind to the calcium channels that govern the flow of calcium across cellular membranes and inactivate them, preventing the influx of calcium and subsequent contraction of vascular tissue. (Richard 2005). Some CCBs may also decrease heart rate and contractility, especially first-generation CCBs (Noll 1998). Blood pressure is decreased as a result.
Numerous sub-types of calcium channels have been identified. L-type channels are dominant through the vascular system and are the target of dihydropyridine CCBs such as amlodipine and nicardipine. Newer agents including manidipine, benzindamine and nilvadipine may act upon T-type channels found in the kidneys, conferring renal protection in comparison to older drugs. Other channels (P/Q type and others) are being investigated as potential therapeutic targets (Hansen 2011).
Adverse effects Peripheral dependent edema is a significant side effect, especially with the use of first- and second-generation CCBs (Burnier 2009). Earlier concerns with increased risk of MI seem to have been associated with large doses of shorter-acting agents rather than drugs in current use (Kaplan 1996). Headaches and flushing are common effects (Makarounas-Kirchmann 2009) in addition to rash, nausea and drowsiness. High-dose verapamil may cause constipation (Elliott 2011).
Calcium channel blockers are used in pregnancy, but a recent retrospective study found an increased risk of infant seizures with pre-term CCB exposure (Davis 2011).
Potential interactions
Plasma levels of cyclosporine and digoxin may be increased by diltiazem and verapamil (Elliott 2011). Many other potential drug-drug interactions exist between CCBs and inhibitors and inducers of CYP3A4. For this reason, CCBs should not be taken with grapefruit juice (Sica 2006a). A recent trial (Koziróg 2011) demonstrated reduced efficacy of nifedipine when used in conjunction with melatonin. Competition for common binding sites may explain this interaction. This drug may also decrease copper levels and increase zinc levels (Misiewicz 1998) but the magnitude and clinical significance of this effect has not been established.
ANGIOTENSIN RECEPTOR BLOCKERS (ARBs)
ARBs are comparatively new additions to the spectrum of hypertensive drugs, with losartan, the first drug in this class, being introduced in 1995 (Sica 2006). Their efficacy appears to be comparable to that of ACE inhibitors (Matchar 2008).
Mechanism of action
Like ACE inhibitors, ARBs affect the RAAS directly, preventing angiotensin II from exerting pressure-increasing effects upon the circulatory system. ARBs are angiotensin II antagonists, binding competitively to type 1 angiotensin receptors and decreasing blood pressure as a result. Some decreases in plasma aldosterone levels may also be anticipated through this effect (Sica 2006).
Adverse effects
In comparison to other antihypertensive agents, ARBs appear to have fewer associated adverse effects (Matchar 2008) and are generally well-tolerated. Notably, ARBs are not associated with a dry cough, unlike ACE inhibitors (Fogari 2011). GI disturbance, fatigue, dizziness, headache and hyperkalemia may present with ARB use (Fogari 2011, Raebel 2011).
Some concerns have been raised recently regarding associations between ARBs and cancer, based upon both meta-analyses (Bangalore 2011, Sipahi 2010) and population studies (Chang 2011). Others have not found evidence of any risk with ARB use (Yoon 2011). Current recommendations advise continued use of ARBs pending further investigation of this link, citing established benefits to cardiovascular health and a lack of conclusive evidence of risk (Rabi 2011, Volpe 2011).
Populations that should not use ARBs include individuals with kidney disease (Sipahi 2010). Acute renal failure may result from use by individuals with renal stenosis (Burnier 2001). ARBs are also not recommended for use in pregnancy (Alwan 2005) although small studies have not shown detriment from early exposure (Diav-Citrin 2011).
Potential interactions
Increased digoxin levels (Elliott 2006) have been reported with ARB use. Other drug-drug interactions are possible. ARBs including valsartan and eprosartan should not be taken with food as this may decrease absorption by up to 40% (Burnier 2001). Like other hypertensive agents, ARBs appear to interact with zinc, promoting excretion and potential deficiency (Koren- Michowitz 2005).
CONCLUSION
Current guidelines encourage the use of pharmacological therapy in the management of hypertension using drugs from the five classes described above. A thorough understanding of mechanisms, interactions and potential adverse effects will encourage safe and effective clinical use of these agents.
References
Alwan S, Polifka JE, Friedman JM. Angiotensin II receptor antagonist treatment during pregnancy. Birth Defects Res A Clin Mol Teratol. 2005 Feb;73(2):123-30.
Bangalore S, Kumar S, Kjeldsen SE, Makani H, Grossman E, Wetterslev J, Gupta AK, Sever PS, Gluud C, Messerli FH. Antihypertensive drugs and risk of cancer: network meta-analyses and trial sequential analyses of 324,168 participants from randomised trials. Lancet Oncol. 2011 Jan;12(1):65-82. Epub 2010 Nov 29.
Barrios V, Calderón A, Navarro-Cid J, Lahera V, Ruilope LM. N-acetylcysteine potentiates the antihypertensive effect of ACE inhibitors in hypertensive patients. Blood Press. 2002;11(4):235-9.
Brixius K, Middeke M, Lichtenthal A, Jahn E, Schwinger RH. Nitric oxide, erectile dysfunction and beta-blocker treatment (MR NOED study): benefit of nebivolol versus metoprolol in hypertensive men. Clin Exp Pharmacol Physiol. 2007 Apr;34(4):327-31.
Burnier M. Angiotensin II type 1 receptor blockers. Circulation. 2001 Feb 13;103(6):904-12. Burnier M, Pruijm M, Wuerzner G. Treatment of essential hypertension with calcium channel blockers: what is the place of lercanidipine? Expert Opin Drug Metab Toxicol. 2009 Aug;5(8):981-7.
Chang CH, Lin JW, Wu LC, Lai MS. Angiotensin receptor blockade and risk of cancer in type 2 diabetes mellitus: a nationwide case-control study. J Clin Oncol. 2011 Aug 1;29(22):3001-7. Epub 2011 Jun 20.
Chrysant SG, Chrysant GS, Dimas B. Current and future status of beta-blockers in the treatment of hypertension. Clin Cardiol. 2008 Jun;31(6):249-52.
Cooper WO, Hernandez-Diaz S, Arbogast PG, Dudley JA, Dyer S, Gideon PS, Hall K, Ray WA.Major congenital malformations after first-trimester exposure to ACE inhibitors. N Engl J Med. 2006 Jun 8;354(23):2443-51.
Crowley SD, Coffman TM. In hypertension, the kidney rules. Curr Hypertens Rep. 2007 Apr;9(2):148- 53.
Davis RL, Eastman D, McPhillips H, Raebel MA, Andrade SE, Smith D, Yood MU, Dublin S, Platt R. Risks of congenital malformations and perinatal events among infants exposed to calcium channel and beta-blockers during pregnancy. Pharmacoepidemiol Drug Saf. 2011 Feb;20(2):138-45. doi: 10.1002/pds.2068. Epub 2010 Nov 15.
Diav-Citrin O, Shechtman S, Halberstadt Y, Finkel-Pekarsky V, Wajnberg R, Arnon J, Di Gianantonio E, Clementi M, Ornoy A. Pregnancy outcome after in utero exposure to angiotensin converting enzyme inhibitors or angiotensin receptor blockers. Reprod Toxicol. 2011 May;31(4):540-5. Epub 2011 Feb 18.
Duarte JD, Cooper-DeHoff RM. Mechanisms for blood pressure lowering and metabolic effects of thiazide and thiazide-like diuretics. Expert Rev Cardiovasc Ther. 2010 Jun;8(6):793-802.
Egom EE, Chirico D, Clark AL. A review of thiazide-induced hyponatraemia. Clin Med. 2011 Oct;11(5):448-51.
Elliott WJ. Drug interactions and drugs that affect blood pressure. J Clin Hypertens (Greenwich). 2006 Oct;8(10):731-7.
Fares A. Night-time exogenous melatonin administration may be a beneficial treatment for sleeping disorders in beta blocker patients. J Cardiovasc Dis Res. 2011 Jul;2(3):153-5
. Fogari R, Zoppi A. A drug safety evaluation of valsartan. Expert Opin Drug Saf. 2011 Mar;10(2):295- 303. Epub 2010 Dec 11.
Francis ME, Kusek JW, Nyberg LM, Eggers PW. The contribution of common medical conditions and drug exposures to erectile dysfunction in adult males. J Urol. 2007 Aug;178(2):591-6; discussion 596. Epub 2007 Jun 13.
Golik A, Zaidenstein R, Dishi V, Blatt A, Cohen N, Cotter G, Berman S, Weissgarten J. Effects of captopril and enalapril on zinc metabolism in hypertensive patients. J Am Coll Nutr. 1998 Feb;17(1):75-8.
Gorre F, Vandekerckhove H.Beta-blockers: focus on mechanism of action. Which beta-blocker, when and why? Acta Cardiol. 2010 Oct;65(5):565-70.
Hansen PB, Poulsen CB, Walter S, Marcussen N, Cribbs LL, Skøtt O, Jensen BL. Functional importance of L- and P/Q-type voltage-gated calcium channels in human renal vasculature. Hypertension. 2011 Sep;58(3):464-70. Epub 2011 Jul 25.
Hayduk K, Kraul H. Efficacy and safety of spirapril in mild-to-moderate hypertension. J Cardiovasc Pharmacol. 1999 Aug;34 Suppl 1:S19-23.
Hines LE, Murphy JE. Potentially harmful drug-drug interactions in the elderly: a review. Am J Geriatr Pharmacother. 2011 Dec;9(6):364-77. Epub 2011 Nov 11. Izzo JL Jr, Weir MR. Angiotensin-converting enzyme inhibitors. J Clin Hypertens (Greenwich). 2011 Sep;13(9):667-75. Epub 2011 Jul 18.
Kaplan NM. The calcium channel blocker controversy. Hypertens Res. 1996 Jun;19(2):57-64. Kendall MJ. Clinical relevance of pharmacokinetic differences between beta blockers. Am J Cardiol. 1997 Nov 13;80(9B):15J-19J.
Kjeldsen K. Hypokalemia and sudden cardiac death. Exp Clin Cardiol. 2010 Winter;15(4):e96-9.
Ko DT, Hebert PR, Coffey CS, Sedrakyan A, Curtis JP, Krumholz HM. Beta-blocker therapy and symptoms of depression, fatigue, and sexual dysfunction. JAMA. 2002 Jul 17;288(3):351-7.
Koizumi K, Ito S. [Hypertension complicated with chronic kidney disease]. Nihon Rinsho. 2011 Nov;69(11):2015-9. [Article in Japanese]
Koren-Michowitz M, Dishy V, Zaidenstein R, Yona O, Berman S, Weissgarten J, Golik A. The effect of losartan and losartan/hydrochlorothiazide fixed-combination on magnesium, zinc, and nitric oxide metabolism in hypertensive patients: a prospective open-label study. Am J Hypertens. 2005 Mar;18(3):358-63.
Koziróg M, Poliwczak AR, Duchnowicz P, Koter-Michalak M, Sikora J, Broncel M. Melatonin treatment improves blood pressure, lipid profile, and parameters of oxidative stress in patients with metabolic syndrome. J Pineal Res. 2011 Apr;50(3):261-6. doi: 10.1111/j.1600-079X.2010.00835.x. Epub 2010 Dec 8.
Krämer BK, Endemann D. [Cardiac risks of hypokalemia and hypomagnesemia]. Ther Umsch. 2000 Jun;57(6):398-9. [Article in German]
Leone A, Landini L, Leone A. Epidemiology and Costs of Hypertension-related Disorders. Curr Pharm Des. 2011;17(28):2955-72.
Luijendijk HJ, van den Berg JF, Hofman A, Tiemeier H, Stricker BH. Beta-blockers and the risk of incident depression in the elderly. J Clin Psychopharmacol. 2011 Feb;31(1):45-50.
Makarounas-Kirchmann K, Glover-Koudounas S, Ferrari P. Results of a meta-analysis comparing the tolerability of lercanidipine and other dihydropyridine calcium channel blockers. Clin Ther. 2009 Aug;31(8):1652-63.
Mas S, Gassò P, Alvarez S, Ortiz J, Sotoca JM, Francino A, Carne X, Lafuente A. Pharmacogenetic predictors of angiotensin-converting enzyme inhibitor-induced cough: the role of ACE, ABO, and BDKRB2 genes. Pharmacogenet Genomics. 2011 Sep;21(9):531-8.
Matchar DB, McCrory DC, Orlando LA, Patel MR, Patel UD, Patwardhan MB, Powers B, Samsa GP, Gray RN. Systematic review: comparative effectiveness of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers for treating essential hypertension. Ann Intern Med. 2008 Jan 1;148(1):16-29. Epub 2007 Nov 5.
Misiewicz A, Jelen B, Dziewit T, Radwan K, Srodon-Sikora I. [Levels of copper, zinc and vitamin C in erythrocytes of humans taking nifedipine]. Pol Arch Med Wewn. 1998 May;99(5):398-402. [Article in Polish]
Nayler WG, Dillon JS. Calcium antagonists and their mode of action: an historical overview. Br J Clin Pharmacol. 1986;21 Suppl 2:97S-107S.
Noll G, Lüscher TF. Comparative pharmacological properties among calcium channel blockers: T-channel versus L-channel blockade. Cardiology. 1998;89 Suppl 1:10-5.
Ott SM, LaCroix AZ, Ichikawa LE, Scholes D, Barlow WE. Effect of low-dose thiazide diuretics on plasma lipids: results from a double-blind, randomized clinical trial in older men and women. J Am Geriatr Soc. 2003 Mar;51(3):340-7.
Patten SB. Propranolol and depression: evidence from the antihypertensive trials. Can J Psychiatry. 1990 Apr;35(3):257-9.
Parish RC, Miller LJ. Adverse effects of angiotensin converting enzyme (ACE) inhibitors. An update. Drug Saf. 1992 Jan-Feb;7(1):14-31.
Piepho RW. Overview of the angiotensin-converting-enzyme inhibitors. Am J Health Syst Pharm. 2000 Oct 1;57 Suppl 1:S3-7.
Rabi DM, Daskalopoulou SS, Padwal RS et al. The 2011 Canadian Hypertension Education Program recommendations for the management of hypertension: blood pressure measurement, diagnosis, assessment of risk, and therapy. Can J Cardiol. 2011 Jul-Aug;27(4):415-433.e1-2.
Raebel MA. Hyperkalemia Associated with Use of Angiotensin-Converting Enzyme Inhibitors and Angiotensin Receptor Blockers. Cardiovasc Ther. 2011 Jan 26. doi: 10.1111/j.1755- 5922.2010.00258.x. [Epub ahead of print]
Ram CV. Beta-blockers in hypertension. Am J Cardiol. 2010 Dec 15;106(12):1819-25. Epub 2010 Nov 2.
Richard S. Vascular effects of calcium channel antagonists: new evidence. Drugs. 2005;65 Suppl 2:1-10.
Robitaille C, Dai S, Waters C, Loukine L, Bancej C, Quach S, Ellison J, Campbell N, Tu K, Reimer K, Walker R, Smith M, Blais C, Quan H. Diagnosed hypertension in Canada: incidence, prevalence and associated mortality. CMAJ. 2011 Nov 21. [Epub ahead of print]
Salort-Llorca C, Mínguez-Serra MP, Silvestre-Donat FJ. Interactions between ibuprofen and antihypertensive drugs: incidence and clinical relevance in dental practice. Med Oral Patol Oral Cir Bucal. 2008 Nov 1;13(11):E717-21.
Salpeter S, Ormiston T, Salpeter E. Cardioselective beta-blockers for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2005 Oct 19;(4):CD003566.
Sarafidis PA, Georgianos PI, Lasaridis AN. Diuretics in clinical practice. Part I: mechanisms of action, pharmacological effects and clinical indications of diuretic compounds. Expert Opin Drug Saf. 2010 Mar;9(2):243-57.
Semple PF. Putative mechanisms of cough after treatment with angiotensin converting enzyme inhibitors. J Hypertens Suppl. 1995 Sep;13(3):S17-21.
Sica DA, Carter B, Cushman W, Hamm L. Thiazide and loop diuretics. J Clin Hypertens (Greenwich). 2011 Sep;13(9):639-43. Epub 2011 Jul 27.
Sica DA. Angiotensin receptor blockers: new considerations in their mechanism of action. J Clin Hypertens (Greenwich). 2006 May;8(5):381-5. Review.
Sica DA. Interaction of grapefruit juice and calcium channel blockers. Am J Hypertens. 2006a Jul;19(7):768-73.
Sipahi I, Debanne SM, Rowland DY, Simon DI, Fang JC. Angiotensin-receptor blockade and risk of cancer: meta-analysis of randomised controlled trials. Lancet Oncol. 2010 Jul;11(7):627-36. Epub 2010 Jun 11.
Stoschitzky K, Sakotnik A, Lercher P, Zweiker R, Maier R, Liebmann P, Lindner W. Influence of beta-blockers on melatonin release. Eur J Clin Pharmacol. 1999 Apr;55(2):111-5.
Takaichi K, Takemoto F, Ubara Y, Mori Y. Analysis of factors causing hyperkalemia. Intern Med. 2007;46(12):823-9. Epub 2007 Jun 15.
Taylor AL, Wright JT Jr. Should ethnicity serve as the basis for clinical trial design? Importance of race/ethnicity in clinical trials: lessons from the African-American Heart Failure Trial (A-HeFT), the African-American Study of Kidney Disease and Hypertension (AASK), and the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). Circulation. 2005 Dec 6;112(23):3654-60; discussion 3666.
Thornton SN. Thirst and hydration: physiology and consequences of dysfunction. Physiol Behav. 2010 Apr 26;100(1):15-21. Epub 2010 Mar 6.
van der Woude HJ, Zaagsma J, Postma DS, Winter TH, van Hulst M, Aalbers R. Detrimental effects of beta-blockers in COPD: a concern for nonselective beta-blockers. Chest. 2005 Mar;127(3):818-24.
Verbeek DE, van Riezen J, de Boer RA, van Melle JP, de Jonge P. A review on the putative association between beta-blockers and depression. Heart Fail Clin. 2011 Jan;7(1):89-99.
Volpe M, Morganti A; Executive Committee of the Italian Society of Hypertension. 2010 position paper of the Italian Society of Hypertension (SIIA): angiotensin receptor blockers and risk of cancer. High Blood Press Cardiovasc Prev. 2011 Mar 1;18(1):37-40.
Wang MT, Su CY, Chan AL, Lian PW, Leu HB, Hsu YJ. Risk of digoxin intoxication in heart failure patients exposed to digoxin-diuretic interactions: a population-based study. Br J Clin Pharmacol. 2010 Aug;70(2):258-67.
Westphal S, Rading A, Luley C, Dierkes J. Antihypertensive treatment and homocysteine concentrations. Metabolism. 2003 Mar;52(3):261-3.
Wiysonge CS, Bradley H, Mayosi BM, Maroney R, Mbewu A, Opie LH, Volmink J. Beta-blockers for hypertension. Cochrane Database Syst Rev. 2007 Jan 24;(1):CD002003.
Wright JM, Musini VM. First-line drugs for hypertension. Cochrane Database Syst Rev. 2009 Jul 8;(3):CD001841.
Yoon C, Yang HS, Jeon I, Chang Y, Park SM. Use of angiotensin-converting-enzyme inhibitors or angiotensin-receptor blockers and cancer risk: a meta-analysis of observational studies. CMAJ. 2011 Oct 4;183(14):E1073-84. Epub 2011 Aug 29.
Carnitine + celecoxib are effective for cancer-related anorexia/cachexia syndrome

A four month, phase III, randomized non-inferiority study was conducted to compare a two-drug combination (carnitine + celecoxib) with carnitine + celecoxib + megestrol acetate for the treatment of cancer-related anorexia/cachexia syndrome (CACS). The primary endpoints were increases of lean body mass (LBM) and improvements of total daily physical activity while the secondary endpoint was an increase in physical performance tested by grip strength and a six-minute walk test (6MWT). Sixty eligible patients were randomly assigned to: arm 1 (L-carnitine 4 g/day + Celecoxib 300 mg/day) or arm 2 (L-carnitine 4 g/day + celecoxib 300 mg/day + megestrol acetate 320 mg/day). All patients received polyphenols 300 mg/day, lipoic acid 300 mg/day, carbocysteine 2.7 g/day, and vitamins A, C, and E. The results did not show a significant difference between treatment arms in both primary and secondary endpoints. Analysis of changes from baseline showed that LBM (determined by dual-energy X-ray absorptiometry and L3 computed tomography) increased significantly in both arms as well as physical performance assessed by 6MWT. Toxicity was quite negligible and comparable between arms. This simple, effective, safe, low cost two-drug approach could be suggested in clinical practice to implement CACS treatment. Clin Nutr. 2011 Oct 31. PMID: 22047681
The current study aimed to investigate whether high serum uric acid (SUA) independently predicts all-cause mortality, cardiovascular mortality, and sudden cardiac death in subjects scheduled for coronary angiography. A total of 3245 individuals enrolled in the Ludwigshafen Risk and Cardiovascular health (LURIC) study were included in the analysis. A total of 730 deaths occurred during the mean follow-up duration of 7.3 (±2.3) years. Among these, cardiovascular diseases and sudden cardiac death accounted for 64.8% and 25.2%, respectively. Adjusting for sex and age, subjects in the fourth SUA quartile had increased all-cause [hazard ratio (HR) = 1.68; p < 0.001] and cardiovascular (HR = 2.00; p < 0.001) mortality compared to individuals in the first quartile. Furthermore, high SUA was a risk factor for sudden cardiac death (HR = 2.27; p < 0.001). These associations remained significant with inclusion of cardiovascular risk factors and the severity of coronary atherosclerosis as covariates in the models. After adjustment for medication use, statistical significance for the association between the SUA quartiles and all-cause mortality disappeared. Therefore, high SUA independently indicated increased risk for cardiovascular and sudden cardiac death in subjects referred for coronary angiography. Nutr Metab Cardiovasc Dis. 2011 Jun 22. PMID: 21703834

The current study was conducted to investigate the relationship between total amylase and metabolic syndrome in 4495 Korean adults who denied any medical history or status of a disorder that could influence their serum amylase. Anthropometry, metabolic risk factors, and total amylase concentration were measured and each participant was categorized into one of four subgroups according to their total amylase concentration. The prevalence of metabolic syndrome by the National Cholesterol Education Program criteria was 13.4%, 15.3%, 19.3%, and 24.2% of those in the fourth, third, second, and lowest quartile of amylase concentration (P for trend < 0.001). After adjusting for age, sex, and body mass index, the odds ratios of the lower quartiles were significantly higher compared to the fourth quartile for the presence of metabolic syndrome. In the receiver-operating characteristics analysis, amylase was similar to uric acid as a significant diagnostic indicator for metabolic syndrome but it had lower diagnostic value than alanine aminotransferase, γ-glutamyltransferase, or C-reactive protein. The authors concluded that lower amylase concentrations are associated with an increased prevalence of metabolic syndrome and that measuring amylase levels may contribute to identifying metabolic syndrome. Clin Chim Acta. 2011 Sep 18;412(19-20):1848-53. PMID: 21726545
Uric acid is predictive of cardiovascular mortality and sudden cardiac death

The current study aimed to investigate whether high serum uric acid (SUA) independently predicts all-cause mortality, cardiovascular mortality, and sudden cardiac death in subjects scheduled for coronary angiography. A total of 3245 individuals enrolled in the Ludwigshafen Risk and Cardiovascular health (LURIC) study were included in the analysis. A total of 730 deaths occurred during the mean follow-up duration of 7.3 (±2.3) years. Among these, cardiovascular diseases and sudden cardiac death accounted for 64.8% and 25.2%, respectively. Adjusting for sex and age, subjects in the fourth SUA quartile had increased all-cause [hazard ratio (HR) = 1.68; p < 0.001] and cardiovascular (HR = 2.00; p < 0.001) mortality compared to individuals in the first quartile. Furthermore, high SUA was a risk factor for sudden cardiac death (HR = 2.27; p < 0.001). These associations remained significant with inclusion of cardiovascular risk factors and the severity of coronary atherosclerosis as covariates in the models. After adjustment for medication use, statistical significance for the association between the SUA quartiles and all-cause mortality disappeared. Therefore, high SUA independently indicated increased risk for cardiovascular and sudden cardiac death in subjects referred for coronary angiography. Nutr Metab Cardiovasc Dis. 2011 Jun 22. PMID: 21703834
Lactobacillus acidophilus NCFM and Bifidobacterium lactis Bi-07 improve bloating in patients with functional bowel disorders

Recent data suggest that intestinal microbiota may play an important role in the pathogenesis of functional bowel disorders. However, probiotic studies in functional bowel disorders have generated inconsistent results thereby suggesting a strain-specific and product-specific effect. To investigate this issue, a probiotic formula containing Lactobacillus acidophilus NCFM (L-NCFM) and Bifidobacterium lactis Bi-07 (B-LBi07) was administered to patients with non-constipating functional bowel disorders twice daily (2×10CFU/day) in this double-blind, placebo-controlled clinical trial over eight weeks (probiotic, n = 31; placebo, n = 29). Primary endpoints were global relief of gastrointestinal symptoms and satisfaction with treatment and secondary endpoints were change in symptom severity, well being, and quality of life. Abdominal bloating improved in the probiotic group compared with the placebo group at four weeks (4.10 vs 6.17, p = 0.009; change in bloating severity p = 0.02) and eight weeks (4.26 vs 5.84, p = 0.06; change in bloating severity P<0.01). The authors concluded that these data support the role of intestinal bacteria in the pathophysiology of functional bowel disorders and that a probiotic formula containing L-NCFM and B-LBi07 may play a role in the management of these disorders. J Clin Gastroenterol. 2011 Jul;45(6):518-25. PMID: 21436726
Elevated alanine aminotransferase is associated with metabolic syndrome

Several studies have suggested that elevated alanine aminotransferase (ALT) is associated with insulin resistance (IR). The health examination profiles of 1313 Taiwanese subjects were investigated cross-sectionally to investigate whether nonspecific elevated ALT could reflect a likely underlying IR and was associated with impaired fasting glucose (IFG) or type 2 diabetes mellitus (T2DM). The prevalence and odds ratios (OR) for IFG/ T2DM and metabolic abnormalities in relation to elevated ALT were analyzed, revealing that subjects with metabolic syndrome (MS) all had IFG/T2DM. The elevated ALT significantly correlated with MS and IFG/T2DM (i.e., 19.9–29.2% vs. 7.8% for MS, and 27.0–31.5% vs. 16.1% for IFG/T2DM). However, after excluding MS and adjustment for age and sex, the elevated ALT alone was not consistently associated with IFG/T2DM (36 < ALT ≤ 80 IU/L with OR 0.97, 95% CI 0.58–1.61; 80 < ALT ≤ 120 IU/L with OR 0.55, 95% CI 0.13–2.37; none with ALT > 120 had IFG). The authors concluded that elevated ALT was associated with MS, but in subjects who did not meet MS criteria, elevated ALT by itself was not associated with IFG/T2DM. Diabetes Res Clin Pract. 2011 Oct;94(1):64-70. PMID: 21715038





