





Five clusters of skin infections have been linked to tattoos in the US. Investigators state that the source of bacteria was the ink itself and although tattoo artists should use sterile water and needles, there is no guarantee of safety if the ink is contaminated. The bacteria that caused these outbreaks of tattoo-related infections are Mycobacterium chelonae and Mycobacterium abscessus, which are common in drinking water. “It’s unfortunate that they can do everything right, but if the manufacturer doesn’t supply them with sterile ink product it still results in them giving their clients infections,” says CDC epidemiologist, Tara MacCannell.
AIDP been granted U.S. patents for MagteinT

AIDP, Inc., the distributors of MagteinTM magnesium L-threonate, has been awarded two patents for magnesium compositions and uses for cognitive function and neurological disorders. Magnesium L-threoate is expected to be the next breakthrough ingredient and these patents protect Magtein’s unique magnesium compositions and its use for any magnesium L-threonate-containing food, nutritional supplements, and drugs for enhancing cognitive function or ameliorating the effects of a neurological disorder.
The use of these products is applicable for improving the health of people suffering from loss of cognitive function, loss of memory, Alzheimer’s disease, depression, attention deficit hyperactivity disorder, Amyotrophic lateral sclerosis (ALS), Parkinson’s disease, migraine, anxiety disorder, and mood disorder, as some examples of cognitive and neurological disorders. “We truly believe that Magtein is a game changing ingredient that will benefit millions of busy and stressed consumers by helping to improve their quality of life,” says Edward Lee Ph.D., AIDP president.
Atrium Innovations announces 2012 second quarter financial results
Atrium Innovations Inc, a globally recognized leader in the development, manufacturing and commercialization of innovative, science-based dietary supplements, released its results for the quarter ending June 30, 2012. Total revenue growth over last year was recorded at 4.1%, or 7.4% on a currency-neutral basis (all organic). Total branded revenue recorded solid organic growth of 12.2%. “We posted solid organic growth on a global basis with a particularly strong performance from our branded products at 12.2%, reflecting solid momentum in the HCP [health care professional] and Retail channels in North America,” said Pierre Fitzgibbon, President and CEO. “Aligned with our right-sizing initiatives, we have decided to close our manufacturing operations in Penticton, British Columbia by the end of September 2012. Production is in the process of being transferred to our other manufacturing facilities.” Mr. Fitzgibbon concluded, “As indicated over the past year, we face heightened pressure from a regulatory perspective. Associated expenses to elevate our cGMP standards have and will continue to impact margins. However, we are seeing evidence that the industry dynamic is changing which will allow overtime recovering part of these regulatory expenses.”
‘Flawed’ JAMA omega-3 meta-analysis may harm public health
The Global Organization of EPA and DHA (GOED) has stated that the new meta-analysis published in JAMA questioning the heart health benefits of omega- 3s is flawed. “Our findings do not justify the use of omega-3 as a structured intervention in everyday clinical practice or guidelines supporting dietary omega-3 PUFA administration,” concluded researchers from the University Hospital of Ioannina in Greece. Adam Ismail, GOED executive director, disputed the findings: “Given the flawed design of this meta-analysis, bypassing the advice of the American Heart Association or the 2010 Dietary Guidelines for Americans by stating that omega-3s are not cardioprotective, could be harmful to public health.” Duffy MacKay, ND, vice president, scientific and regulatory affairs for the Council for Responsible Nutrition (CRN) added that many of the studies included in the meta-analysis were conducted on diseased individuals already undergoing treatment with one or more drugs (e.g., statins), which may mask the less potent and more long-term effects of omega-3 fats. “Along these lines, the researchers apparently did not examine within each individual study included in the meta-analysis whether individuals in the placebo group were sufficient or insufficient in their dietary intake omega-3 fats. Without that information, they could not have controlled for this variable.”
Dr Kristy Prouse, MD, FRCSC

Dr Kristy Prouse, MD, FRCSC Institute for Hormonal Health
IHP has had the privilege of interviewing what has now been dozens of conventionally- trained physicians who at some point in their career make the decision to adopt integrative systems of practice. Each of these stories unfolds with unique circumstances, yet they all seem to share a stunning number of similarities. Dr Kristy Prouse, MD, FRCSC is a welcomed addition to the growing list of conventionally- trained Canadian physicians finding answers to difficult medical questions among the trainings of integrative healthcare providers.

Dr. Andrea Kuzmiski ND,
Kristina Graham HN,
Michelle Armstrong CPT,
Dr. Kristy Prouse MD, FRCSC, Ashna Starrett HHP,Camille Lawson RN
After many years of conventional practice as an OBGYN, performing several thousand deliveries and gynecological surgeries, Kristy felt she was lacking adequate tools to help a large and growing number of her patients. Training that included bioidentical hormone therapy, an understanding of the concept of adrenal fatigue, nutrition and nutraceutical science, and herbal medicines has seen her transform her career into something her colleagues from the past remain confused by. Welcome to the practice of integrative medicine Kristy. As yet another conventionally- trained physician we interviewed once stated “once you start using this type of medicine, you find yourself ethically unable to go back”.
Dr Prouse began her academic training in 1998 with a degree in Psychology from Western University. She obtained a second undergraduate degree in Genetics and Cell Biology from the University of Toronto, then went on to complete medical training at Queen’s University. In 1988 Kristy began her medical residency at the University of Calgary in Obstetrics and Gynecology, where she received the Laparoscopic Surgery Award of Excellence. In 2002 Kristy entered her first practice, in Orillia, Ontario. This “smaller” town setting was a general OBGYN practice. Two years later, Kristy moved to the Trillium Health Centre in Mississauga, to be closer to her ailing mother. She maintained her position at the Trillium Health Centre, and simultaneously took on roles of Associate Professor at the University of Toronto School of Medicine and the Northern Ontario School of Medicine. Kristy maintained her role at the Trillium Health Centre until October of 2011, opening the Institute for Hormonal Health, in Oakville, Ontario, in November of 2011.
 What led this well- decorated, successful, mother of twin 11 year old girls, OBGYN to leave the Trillium Health Centre in favour of opening her own model of integrative health centre? As has often been the case, Dr Prouse’s story begins with a personal health crisis. “There was a lot happening at once… the demands of practice at the Trillium centre… frustration with aspects of the care I was providing people… feeling I didn’t have good answers for a lot of the concerns my patients had… Then realizing I was in need of the same solutions my patients were seeking! By early 2011, I was simply burnt out! I started thinking of ways to manage my situation, but did so not knowing a different medical model may have a solution for me. My answers were to consider practicing half time, perhaps bringing a colleague on board to share a practice with, and I was even considering outright retirement”. Kristy goes on to describe “after having considered visiting an integrative healthcare provider for some time, a set of unique circumstances arose where a specific integrative healthcare provider was suggested to me as someone to see on four separate occasions within a 48 hour period! I was diagnosed as having “adrenal fatigue”… I felt better within days of initiating treatment”.
What led this well- decorated, successful, mother of twin 11 year old girls, OBGYN to leave the Trillium Health Centre in favour of opening her own model of integrative health centre? As has often been the case, Dr Prouse’s story begins with a personal health crisis. “There was a lot happening at once… the demands of practice at the Trillium centre… frustration with aspects of the care I was providing people… feeling I didn’t have good answers for a lot of the concerns my patients had… Then realizing I was in need of the same solutions my patients were seeking! By early 2011, I was simply burnt out! I started thinking of ways to manage my situation, but did so not knowing a different medical model may have a solution for me. My answers were to consider practicing half time, perhaps bringing a colleague on board to share a practice with, and I was even considering outright retirement”. Kristy goes on to describe “after having considered visiting an integrative healthcare provider for some time, a set of unique circumstances arose where a specific integrative healthcare provider was suggested to me as someone to see on four separate occasions within a 48 hour period! I was diagnosed as having “adrenal fatigue”… I felt better within days of initiating treatment”.
 This personal journey led Kristy to dedicate countless hours to literature- based research on the concept of adrenal fatigue, which then spurred interest in the much larger spectrum of practice that comprises integrative medicine. Kristy felt that what she was finding was the solution to the many problems she had seen in years of practice as an OBGYN that she had no solution for. She described a sense of the system of practice being much more in alignment with her person… “alignment with what I was meant to be doing”… Since making the transition to an integrative system of practice Kristy feels renewed. “Recognizing patterns in history and physical examination as well as implementing objective testing has me using my brain in a way I haven’t in years! The most rewarding part however is effecting significant change for many people who are seeking our help after exhausting their options in the conventional system and after being told that there is nothing wrong with them.”
This personal journey led Kristy to dedicate countless hours to literature- based research on the concept of adrenal fatigue, which then spurred interest in the much larger spectrum of practice that comprises integrative medicine. Kristy felt that what she was finding was the solution to the many problems she had seen in years of practice as an OBGYN that she had no solution for. She described a sense of the system of practice being much more in alignment with her person… “alignment with what I was meant to be doing”… Since making the transition to an integrative system of practice Kristy feels renewed. “Recognizing patterns in history and physical examination as well as implementing objective testing has me using my brain in a way I haven’t in years! The most rewarding part however is effecting significant change for many people who are seeking our help after exhausting their options in the conventional system and after being told that there is nothing wrong with them.”

Kristy has managed to assemble an incredible team of integrative healthcare providers, each brining a unique skillset to complement the team as a whole. Dr Andrea Kuzmiski, ND, a 2004 graduate of the Canadian College of Naturopathic Medicine, certified in parenteral therapy, is described as a key member of the team. Among the broad set of skills Andrea is able to showcase in the facility, Kristy highlights the immense value of parenteral therapies, especially for what is described as advanced stages of adrenal fatigue. The Institute for Hormonal Health team also includes Kristina Graham, holistic nutritionist, Michelle Armstrong, personal trainer and wellness counselor, Ashna Starett, holistic health practitioner, and Camille Lawson, sex therapist.

Many centres of integrative healthcare attempt to duplicate the IHH model of care delivery, yet most fail to do so. Jennine Le Tendre acts as the patient care coordinator. A patients first and second visit are booked with Dr Prouse. A portion of these visits is OHIP covered, dealing with the taking of the case history and physical exam. There is also a fee for service for patient visits, as well as fees for integrative tests performed, etc… Integrative testing is often recommended, the specific test(s) chosen based on the case presentation. The second visit with Dr Prouse provides an opportunity for the patient to review the findings of the intake, physical exam, and results of integrative testing, and to decide upon the best course of treatment. Jennine plays a vital role serving as the patient’s point of contact, educating patients as to the use of integrative diagnostic test kits, and coordinating future patient visits to the team members best suited for the specific case in question. The IHH achieves a truly integrative model of care, with Kristy serving as the medical coordinator and Jennine serving as the patient coordinator for each case.
 I asked Kristy about the reaction of her colleagues to the news that she would be leaving the Trillium Health Centre to open a private integrative medical practice. She replied “they were supportive and excited for me, but somewhat uninterested in what I was going to be doing”. That got me thinking… I have met many hundreds, thousands in fact, of conventionally- trained MD’s who have never read a thing about integrative medicine, but are convinced it is a useless practice. Each and every MD who spends even 10 hours reading about integrative medicine invariably ends up at the same place; reading more about integrative medicine. And after enough hours of reading, such MD’s either practice integrative medicine themselves, or partner with integrative healthcare practitioners to make such care available to their patients. So we seem to be evolving to a solution… We need to expose MD’s to evidence pertaining to integrative medicine… “One MD at a time” seems to be working quite well, as the number of conventionally- trained MD’s taking up practice as integrative healthcare providers is growing exponentially. It seems we are approaching a tipping point… How long can it possibly be until true integrative medicine makes its way into medical school curriculums?
I asked Kristy about the reaction of her colleagues to the news that she would be leaving the Trillium Health Centre to open a private integrative medical practice. She replied “they were supportive and excited for me, but somewhat uninterested in what I was going to be doing”. That got me thinking… I have met many hundreds, thousands in fact, of conventionally- trained MD’s who have never read a thing about integrative medicine, but are convinced it is a useless practice. Each and every MD who spends even 10 hours reading about integrative medicine invariably ends up at the same place; reading more about integrative medicine. And after enough hours of reading, such MD’s either practice integrative medicine themselves, or partner with integrative healthcare practitioners to make such care available to their patients. So we seem to be evolving to a solution… We need to expose MD’s to evidence pertaining to integrative medicine… “One MD at a time” seems to be working quite well, as the number of conventionally- trained MD’s taking up practice as integrative healthcare providers is growing exponentially. It seems we are approaching a tipping point… How long can it possibly be until true integrative medicine makes its way into medical school curriculums?
IHP is grateful to Dr Kristy Prouse and the entire Institute for Hormonal Health team for taking the time to allow us to showcase their efforts to you. A conventionally- trained OBGYN felt the care she was providing was lacking, improved her own health through visits to an integrative healthcare provider, and subsequently evolved her own career to mirror the lessons she learned through research and a personal healing journey. After five years of delivering IHP this is somewhat of a broken record, yet one we love hearing over and over again.
Mahaya Forest Hill Integrative Clinic

Mahaya Forest Hill Integrative Clinic
We at IHP are pleased to introduce the innovative Mahaya Forest Hill Integrative Health clinic. This integrative clinic is a multi-disciplinary wellness centre located in the beautiful Forest Hill neighbourhood in Toronto, near St. Clair Avenue West and Avenue Road. It opened its doors in 2010 as an expansion of the original downtown Mahaya clinic and was taken over by new management in June 2012. Since that time, it has been run successfully and independently by its new owner and Clinic Director, Dr. Chris Habib, ND.
After his graduation at the Canadian College of Naturopathic Medicine, Chris proceeded to become the first and only person in Canada to complete an accredited two-year research residency. Chris has always had a passion for promoting integrative medicine and saw this clinic as an opportunity to further his goal on a larger scale. Since the transition in ownership, Chris has made it his mission to provide the community with unparalleled integrative health services. The clinic treats all of its patients with the utmost respect and strives to ensure that every single patient receives the absolute highest quality of care. All aspects of the patient interaction are taken into consideration so that patients are provided with the best possible overall health experience.

Mahaya Forest Hill is located on the ground floor of a house at the corner intersection of a residential street and St. Clair Avenue West, creating a cozy and professional atmosphere for patients. Free parking is available on-site and the clinic is easily accessible by TTC. There is also a dentist, an esthetician, a counsellor, and a psychotherapist working out of the same building. The clinic benefits from the traffic of these and neighbouring businesses, as well as the street traffic on St. Clair Avenue West. Mahaya Forest Hill is a proud member of the Toronto Midtown Business Association and connects with the business community by providing talks at local companies. They also connect with the community through a strong social media presence, including blogging, newsletters, Facebook, Twitter, and LinkedIn. Chris’ wife, Nicole Habib, works behind-the-scenes as the Marketing Director of the clinic, bringing with her marketing experience from the publishing industry.
The strength of Mahaya Forest Hill lies in its unique team of diverse health care practitioners. The team currently includes six Naturopathic Doctors, three Registered Massage Therapists, two Chiropractors, one Osteopath, and one Acupuncturist. On any given day of the week, patients have access to a specialized team of practitioners who work together to provide optimal wholeperson treatments. All health teams include at least one Naturopathic Doctor who ensures long-term health and works with the patient to optimize diet, nutrition, lifestyle, and address any other health factors. Together, the practitioners also make certain that the body is working properly from a structural perspective and that any pain is treated effectively through a variety of therapies. Overall, the practitioners have a tremendous amount of education and also have additional training in some of the following areas: evidence-based medicine, women’s health, acupuncture, blood typing, Arvigo massage, homeopathy, orthotic assessments, doula training, manual lymph drainage, and combined decongestive therapy.
Patients are often introduced to the clinic through one initial contact point, whether it be with an individual practitioner or through the clinic’s website. All practitioners offer free 15-minute consultations to discuss their services with prospective patients. After booking an initial visit and working with one practitioner, patients have the option to expand their health team. Practitioners are responsible for making sure their patients obtain thorough care and this usually entails going beyond their own scope of practice. As a result, the clinic incorporates specialized inter-referral forms so that the entire health team has full access to all pertinent health information. From that point, patients are able to schedule back-to-back appointments with different practitioners, which provides them with an extremely supportive health experience. One specific goal of the clinic is to make this type of health care more accessible and so the clinic is open for extended hours Monday to Saturday.



Patients can also take advantage of specific programs that are offered by the clinic. The various programs provide support through different life stages and through natural life transitions. These programs include the Healthy Breast, Healthy Conception, Detoxification, Facial Rejuvenation, Healthy Weight Loss, Healthy Menopause, Healthy Pregnancy, Optimal Prevention, and Cancer Care.
The clinic includes a laboratory with state-of-the-art integrative diagnostics and a dispensing room. Both on-site and and off-site blood draws are available for patients. Mahaya Forest Hill utilizes Gamma Dynacare, Rocky Mountain Analytical, ImmunoLabs, and Metametrix among some of its lab service providers. The supplement dispensary consists of a wide variety of the highest quality nutraceuticals, botanicals, topical creams, and homeopathics from companies such as AOR, NFH, Seroyal, Thorne, EBI, Boiron, St Francis Herb Farm, Promedics, and Douglas Labs. In addition, the clinic also carries specially formulated tinctures by Etheric Herbals and a large collection of dried herbs and teas. Custom herbal formulas can also be created for patients to address their individual health needs.
IHP would like to thank Mahaya Forest Hill for the opportunity to highlight this highly successful clinic. Having many practitioners in one facility does not in itsellf define a multidisciplinary practice; it is the interaction between the allied practitioners, and their ability to effectively manage patient care in a manner that maximizes the unique skillset of the specific practitioners. Mahaya Forest Hill has achieved an impressive balance in delivery of truly integrative and multidisciplinary healthcare

Intravenous Therapies

Intravenous Therapies
Fish oil based lipid emulsions (FOBLE)
Fish oil based lipid emulsions (FOBLE) have an excellent record of safe and effective use, objectively evaluated in over 55 human intervention trials. Critical care hospital settings remain the most thoroughly evaluated areas of their application, however interest in management of flares of chronic inflammatory disorders such as arthritis and psoriasis has begun to emerge. By showcasing the clinical utility of this safe and effective intravenous treatment strategy, it is hoped, progress can be made in adding fish oil to the armament of intravenous therapies at the disposal of integrated healthcare providers.
Introduction
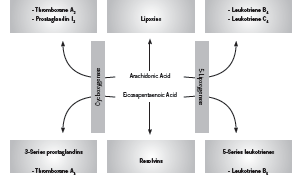
Fish derived omega-3 (n-3) fatty acids, specifically eicosapentanoic acid (EPA) and docosahexanoic acid (DHA) are well recognized for their anti-inflammatory effects (Rangel-Huerta 2012). Upon incorporation into the cell membrane, EPA and DHA competitively inhibit production of pro-inflammatory cytokines from arachidonic acid (AA), such as prostaglandin E2 (PGE2), and serve as a substrate for production of less active prostaglandin E3 (PGE3, anti-inflammatory) (Mayer 2006). In addition, EPA and DHA are precursors for the inflammation-resolving mediators appropriately known as resolvins (Calder 2010). The uses of intravenously (IV) administered fish oils, or fish oil based lipid emulsions (FOBLE), are lesser known. Nonetheless, there is a welldeveloped body of research demonstrating impressive clinical benefits associated with use of IV fish oils. The most supported application of IV fish oils is in the critical care setting, however other areas of application have also been investigated. Figure 1 shows the effect of EPA on generation of inflammatory cytokines.
A Pubmed search for “intravenous omega-3” on 10 August 2012 yielded 57 clinical trials. Not all of these are included here since some pertain to highly specialized applications, such as liver disease in premature infants, total parenteral (TPN) –related liver disease, endstage renal disease, or biomarker studies such as those investigating effects on antioxidant status. This article includes 18 clinical trials of intravenous omega-3 fatty acids related to the following areas: 1) critical care (n=13); 2) rheumatoid arthritis (n=2); and 3) psoriasis and inflammatory skin diseases (n=3).
Pharmacology
The most widely used and well-researched parenteral lipid emulsion featuring omega-3 fatty acids is Omegaven (Fresenius-Kabi, Germany). Omegaven is a 10% fish oil emulsion meaning that it contains 10g refined fish oil per 100mL, including between 1-3g each EPA and DHA (Calder 2010, Fresenius Kabi 2010). Other fish oil based formulations include SMOFLipid 20% (Fresenius-Kabi), which contains 30g total fish oils per 1000mL in combination with soybean oil, medium chain triglycerides, and olive oil (AusPAR 2010, Calder 2010); and Lipoplus (B. Braun, Germany), which contains 20g total fish oil per 1000mL in combination with soybean oil and medium chain triglycerides (B. Braun un-dated product information).
Intravenous delivery of n-3 PUFAs has been shown to circumvent the slower n-3 incorporation into phospholipid membranes following oral administration (Carpentier 2010, Roulet 1997, Simeons 2008). Incorporation of EPA into leukocyte and platelet membranes after IV administration occurs within 60 minutes (Carpentier 2010). Similarly, Madsen found that IV administration of 4.1g n-3 PUFAs (polyunsaturated fatty acids) resulted in an increase of levels present in platelet phospholipids at 4 hours, and increased levels in plasma phospholipids at 48 hours, while there was no change in the placebo group (2011).
A study by Roulet conducted among 10 postoperative patients found that a lipid emulsion with 10% fish oil added resulted in a greater than two-fold increase in the EPA content of platelet phospholipids, and decreased maximal platelet reaction speed (p <0.02) while increasing latency (p <0.002), indicating a less heightened immune response (1997). Importantly, no toxicities, including no increase in postoperative bleeding and no abnormalities in hepatic and renal function, were observed during the fish oil infusion (Roulet 1997). Pradier et al investigated the safety of a bolus IV injection of a medium-chain triglyceride:fish oil emulsion (8:2 ratio) on hemostatic parameters in 12 healthy subjects (2008). No adverse effect was found on 1) occlusion time in response to the ADP (adenosine diphosphate, a platelet activator) or the epinephrine test; 2) levels of certain markers of coagulability, such as fibrinogen, PAC-1, and others, in response to ADP, collagen or thrombin receptor analog peptide six when examined ex vivo. Authors concluded that these results support the hemostatic safety of the IV fish oil emulsion (Pradier 2008).
Clinical trials
Critical Care: Sepsis and Systemic Inflammatory Response Syndrome (SIRS) In the critical care setting, intravenous supplementation with fish oil is being studied for its powerful immunologic effects (Mayer 2006). In particular, IV fish oil has been shown to decrease the length of hospitalization in patients undergoing abdominal surgery (Jiang 2010), decrease levels of inflammation in patients with sepsis or SIRS (Sungertekin 2011), and decrease complications in post-operative patients (Heller 2006). For years, the standard lipid based emulsion used in patients requiring total or partial parenteral nutrition (TPN, PN) has consisted of soybean oil rich in omega-6 fatty acids (Mayer 2006). It was subsequently found however that high amounts of omega-6 fatty acids may in fact harmfully suppress immune function, resulting in increased rates of infection (Calder 2010, Nordenström 1979, Snydman 1982). Conversely, newer emulsions such as Omegaven containing 10% (w/v) fish oil have been shown to beneficially impact immune function in healthy (Pittet 2010, Pluess 2007) and hospitalized patients (Wei 2010).
In healthy patients, Omegaven has been shown to blunt the immune response to the endotoxin lipopolysaccharide (LPS) (Pittet 2010, Pluess 2007). Since bacterial-derived LPS acts as a trigger eliciting many of the harmful symptoms of infection and/ or sepsis essentially effected by the immune system, such as fever, systemic inflammation, and shock, reducing this reaction is considered beneficial in these patients. In addition, Pluess et al found that Omegaven blunted the effects of LPS on fever and the neuroendocrine response to infection (2007).
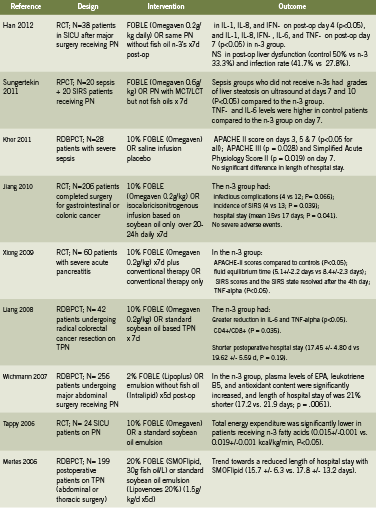
Patients
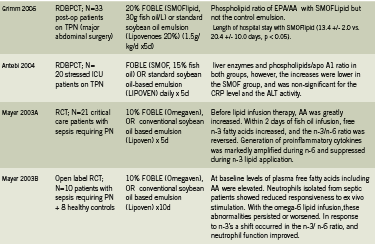
chain triglyceride; MCT medium chain triglyceride; NS non significant; PN parenteral nutrition; SICU surgical intensive
care unit; TPN total parenteral nutrition.
Table 1 presents a summary of 13 human trials investigating use of IV fish oil in critical care patients for outcomes related to sepsis, systemic inflammatory response syndrome (SIRS, syndrome secondary to severe infection), hospitalization, and mortality. These studies show that use of FOBLE may: improve post-operative liver function and rates of infection (Han 2012); improve Acute Physiology and Chronic Health Evaluation (APACHE) scores, a disease severity scoring system used in ICU settings, in patients with severe sepsis (Khor 2011) and pancreatitis (Xiong 2009); prevent infectious complications and incidence of SIRS, and reduce hospital stays in cancer patients undergoing major abdominal surgery (Jiang 2008, Liang 2008).
In addition, a 2010 meta analysis reviewed six RCTs conducted in Europe and Asia that compared parenteral nutrition with or without fish oil emulsion in postoperative patients (Wei 2010). Although in this study there was no significant impact on mortality, use of fish oil was associated with a significant reduction in infectious complications (relative risk RR 0.49, 95% confidence interval 0.26-0.93, P=0.03). The length of hospital stay was non-significantly decreased by over 3 days, with a decrease in 2.07 days in the intensive care unit (Wei 2010).
A prospective study of Omegaven among 661 patients with major abdominal surgery, abdominal sepsis, nonabdominal sepsis, serious trauma, or other diagnoses, and receiving TPN for three days or more, in 82 German hospitals, found that use of FOBLE resulted in: favorable effects on survival, infection rates, and length of stay, when administered in doses between 0.1 and 0.2 g/kg/day (Heller 2006). At doses of 0.15-0.2 g/kg/day, antibiotic requirements were 26% lower when compared with doses of <0.05 g/kg/day. After peritonitis and abdominal sepsis, the fish oil dose for minimizing length of intensive care unit stay was 0.23 g/kg/day (Heller 2006).
Rheumatoid Arthritis
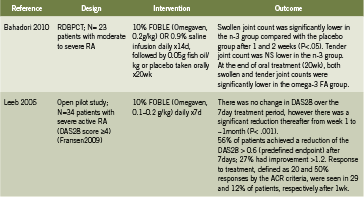
Table 2 summarizes two human trials investigating IV fish oil emulsions in the treatment of active rheumatoid arthritis (RA) (Bahadori 2010, Leeb 2006). In a randomized, double blind, placebo controlled trial, Bahadori administered IV fish oil 0.2g/kg daily for 14 days in patients with moderate to severe RA, followed by oral fish oil for 20 weeks, and found that after only one week, as well as after two weeks, swollen joint count was significantly lower in the fish oil group (2010). This effect persisted to the end of 20 weeks/ end of oral supplementation as well. Leeb conducted an open pilot trial in patients with severe RA, administering 0.1-0.2g/ kg fish oil daily for seven days; there was a significant reduction in disease severity ratings over time (p<0.001) and tolerability was rated as “excellent” (Leeb 2006). Intravenous fish oil may represent a safe and rapidly acting strategy to control severe acute RA.
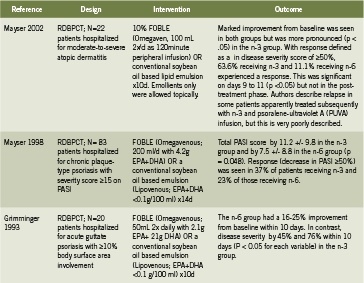
Dermatology: Psoriasis and Atopic Dermatitis Table 3 summarizes three human trials investigating IV fish oil emulsions for the treatment of psoriasis or atopic dermatitis (Grimminger 1993, Mayser 2002, Mayser 1998). In patients with moderate to severe atopic dermatitis, IV fish oil for 10 days resulted in significant improvement in disease severity (visible by day 6) (p<0.05) compared to placebo (Mayser 2002). An earlier study by the same team examined patients hospitalized for chronic plaque type psoriasis (Mayser 1998). Treatment with Omegaven for 14 days resulted in significant reduction in the Psoriasis Activity Severity Index (PASI) (p=0.048) in the fish oil group compared to controls. A total of 16 of 43 patients (37%) in the fish oil group experienced a clinical response, defined as a reduction in PASI of 50% or greater, compared to 23% in the control group.
Finally, Grimminger found that IV fish oil improved disease severity between 45- 76% depending on the scoring measure (p<0.05 for all) in hospitalized patients with psoriasis involving 10% or more of their body surface area (1993). Remarkably, the treatment effect was evident within four to seven days of daily IV fish oil administration. Finally, IV fish oils have been shown to reduce cardiac arrhythmias (Heidt 2009) and improve PN-associated liver disease (Le 2010), however these applications are beyond the scope of this paper.
Conclusion
Intravenously administered fish-derived omega-3 fatty acids have been studied for a number of indications including the treatment and prevention of serious infection and SIRS in hospitalized patients; treatment of acute rheumatoid arthritis; inflammatory skin conditions including psoriasis and atopic dermatitis; as well as the prevention of arrhythmias and liver disease. In these populations, IV fish oil has been demonstrated to improve immune function, shorten hospitalization, reduce mortality, and significantly decrease disease activity. In some cases, the rate of disease improvement is rapid, occurring within the first week of treatment. Although parenteral fish oil emulsions are not currently available to NDs, we hope that access to this safe and efficacious agent will be broadened in the future
Key: PASI Psoriasis Area and Severity Index; RCT randomized controlled trial; RDBPCT randomized double blind
placebo controlled trial;
References
Antébi H, Mansoor O, Ferrier C, Tétégan M, Morvan C, Rangaraj J, Alcindor LG. Liver function and plasma antioxidant status in intensive care unit patients requiring total parenteral nutrition: comparison of 2 fat emulsions. JPEN J Parenter Enteral Nutr. 2004 May-Jun;28(3):142-8.
AusPAR: Australian Public Assessment Report for SMOF Lipid. Product Information. June 2010. www.tga.gov.au/pdf/auspar/ausparsmoflipid. pdfAccessed 29 August 2012.
Bahadori B, Uitz E, Thonhofer R, Trummer M, Pestemer-Lach I, McCarty M, Krejs GJ. Omega-3 Fatty acids infusions as adjuvant therapy in rheumatoid arthritis.JPEN J Parenter Enteral Nutr. 2010 Mar-Apr;34(2):151-5.
B. Braun. Clinical Nutrition Short Guide, Lipoplus Product Information. http://www.bbraun.com/documents/Knowledge/Short_ Guide_Clinical_Nutrition.pdf Accessed 29 August 2012.
Calder PC, Jensen GL, Koletzko BV, Singer P, Wanten GJ. Lipid emulsions in parenteral nutrition of intensive care patients: current thinking and future directions. Intensive Care Med. 2010 May;36(5):735-49.
Calder PC. Hot topics in parenteral nutrition. Rationale for using new lipid emulsions in parenteral nutrition and a review of the trials performed in adults. ProcNutr Soc. 2009 Aug;68(3):252-60.
Carpentier YA, Hacquebard M, Portois L, Dupont IE, Deckelbaum RJ, Malaisse WJ. Rapid cellular enrichment of eicosapentaenoate after a single intravenous injection of a novel medium-chain triacylglycerol:fish-oil emulsion in humans. Am J ClinNutr. 2010 Apr;91(4):875-82.
de Meijer VE, Gura KM, Meisel JA, Le HD, Puder M. Parenteral fish oil monotherapy in the management of patients with parenteral nutrition-associated liver disease. Arch Surg. 2010 Jun;145(6):547-51.
Fallon EM, Le HD, Puder M. Prevention of parenteral nutritionassociated liver disease: role of omega-3 fish oil. CurrOpin Organ Transplant. 2010 Jun;15(3):334-40.
Fransen J, van Riel PL. The Disease Activity Score and the EULAR response criteria. Rheum Dis Clin North Am. 2009 Nov;35(4):745- 57, vii-viii.
Fresenius Kabi New Zealand Ltd. Consumer Medicine Information for Omegaven. July 2010. www.medsafe.govt.nz/consumers/cmi/o/ omegaven.pdfAccessed 29 August 2012.
Grimm H, Mertes N, Goeters C, Schlotzer E, Mayer K, Grimminger F, Fürst P. Improved fatty acid and leukotriene pattern with a novel lipid emulsion in surgical patients. Eur J Nutr. 2006 Feb;45(1):55-60.
Grimminger F, Mayser P, Papavassilis C, Thomas M, Schlotzer E, Heuer KU, Führer D, Hinsch KD, Walmrath D, Schill WB, et al. A double-blind, randomized, placebo-controlled trial of n-3 fatty
acid based lipid infusion in acute, extended guttate psoriasis. Rapid improvement of clinical manifestations and changes in neutrophil leukotriene profile.ClinInvestig. 1993 Aug;71(8):634-43.
Han YY, Lai SL, Ko WJ, Chou CH, Lai HS.Effects of fish oil on inflammatory modulation in surgical intensive care unit patients. NutrClinPract. 2012 Feb;27(1):91-8.
Heidt MC, Vician M, Stracke SK, Stadlbauer T, Grebe MT, Boening A, Vogt PR, Erdogan A. Beneficial effects of intravenously administered N-3 fatty acids for the prevention of atrial fibrillation after coronary artery bypass surgery: a prospective randomized study. ThoracCardiovasc Surg. 2009 Aug;57(5):276-80.
Heller AR, Rössler S, Litz RJ, Stehr SN, Heller SC, Koch R, Koch T. Omega-3 fatty acids improve the diagnosis-related clinical outcome. Crit Care Med. 2006 Apr;34(4):972-9.
Jiang ZM, Wilmore DW, Wang XR, Wei JM, Zhang ZT, Gu ZY, Wang S, Han SM, Jiang H, Yu K. Randomized clinical trial of intravenous soybean oil alone versus soybean oil plus fish oil emulsion after gastrointestinal cancer surgery. Br J Surg. 2010 Jun;97(6):804-9.
Khor BS, Liaw SJ, Shih HC, Wang LS. Randomized, double blind, placebo-controlled trial of fish-oil-based lipid emulsion infusion for treatment of critically ill patients with severe sepsis. Asian J Surg. 2011 Jan;34(1):1-10.
Le HD, de Meijer VE, Zurakowski D, Meisel JA, Gura KM, Puder M. Parenteral fish oil as monotherapy improves lipid profiles in children with parenteral nutrition-associated liver disease. JPEN J Parenter Enteral Nutr. 2010 Sep-Oct;34(5):477-84.
Leeb BF, Sautner J, Andel I, Rintelen B. Intravenous application of omega-3 fatty acids in patients with active rheumatoid arthritis. The ORA-1 trial.An open pilot study. Lipids. 2006 Jan;41(1):29-34.
Liang B, Wang S, Ye YJ, Yang XD, Wang YL, Qu J, Xie QW, Yin MJ. Impact of postoperative omega-3 fatty acid-supplemented parenteral nutrition on clinical outcomes and immunomodulations in colorectal cancer patients.World J Gastroenterol. 2008 Apr 21;14(15):2434-9.
Madsen T, Christensen JH, Thøgersen AM, Schmidt EB, Toft E. Intravenous infusion of n-3 polyunsaturated fatty acids and inducibility of ventricular tachycardia in patients with implantable cardioverter defibrillator. Europace. 2010 Jul;12(7):941-6.
Madsen T, Christensen JH, Toft E, Aardestrup I, Lundbye- Christensen S, Schmidt EB. Effect of intravenous omega-3 fatty acid infusion and hemodialysis on fatty acid composition of free fatty acids and phospholipids in patients with end-stage renal disease. JPEN J Parenter Enteral Nutr. 2011 Jan;35(1):97-106.
Mayer K, Schaefer MB, Seeger W. Fish oil in the critically ill: from experimental to clinical data. CurrOpinClinNutrMetab Care. 2006 Mar;9(2):140-8.
Mayer K, Gokorsch S, Fegbeutel C, Hattar K, Rosseau S, Walmrath D, Seeger W, Grimminger F. Parenteral nutrition with fish oil modulates cytokine response in patients with sepsis. Am J RespirCrit Care Med. 2003 May 15;167(10):1321-8. A
Mayer K, Fegbeutel C, Hattar K, Sibelius U, Krämer HJ, Heuer KU, Temmesfeld-Wollbrück B, Gokorsch S, Grimminger F, Seeger W. Omega-3 vs. omega-6 lipid emulsions exert differential influence on neutrophils in septic shock patients: impact on plasma fatty acids and lipid mediator generation. Intensive Care Med. 2003 Sep;29(9):1472-81. B
Mayser P, Mayer K, Mahloudjian M, Benzing S, Krämer HJ, Schill WB, Seeger W, Grimminger F. A double-blind, randomized, placebocontrolled trial of n-3 versus n-6 fatty acid-based lipid infusion in atopic dermatitis. JPEN J Parenter Enteral Nutr. 2002 May- Jun;26(3):151-8.
Mayser P, Mrowietz U, Arenberger P, Bartak P, Buchvald J, Christophers E, Jablonska S, Salmhofer W, Schill WB, Krämer HJ, Schlotzer E, Mayer K, Seeger W, Grimminger F. Omega-3 fatty acid-based lipid infusion in patients with chronic plaque psoriasis: results of a double-blind, randomized, placebo-controlled, multicenter trial. J Am AcadDermatol. 1998 Apr;38(4):539-47.
Mertes N, Grimm H, Fürst P, Stehle P. Safety and efficacy of a new parenteral lipid emulsion (SMOFlipid) in surgical patients: a randomized, double-blind, multicenter study. Ann NutrMetab. 2006;50(3):253-9.
Park KT, Nespor C, Kerner J Jr. The use of Omegaven in treating parenteral nutrition-associated liver disease. J Perinatol. 2011 Apr;31Suppl 1:S57-60.
Pluess TT, Hayoz D, Berger MM, Tappy L, Revelly JP, Michaeli B, Carpentier YA, Chioléro RL. Intravenous fish oil blunts the physiological response to endotoxin in healthy subjects. Intensive Care Med. 2007 May;33(5):789-97.
Nordenström J, Jarstrand C, Wiernik A. Decreased chemotactic and random migration of leukocytes during Intralipid infusion. Am J Clin Nutr. 1979 Dec;32(12):2416-22.
Pradier O, Portois L, Malaisse WJ, Carpentier YA. Hemostatic safety of the bolus intravenous injection of a novel medium-chain triglyceride:fish oil emulsion. Int J Mol Med. 2008 Sep;22(3):301-7.
Rangel-Huerta OD, Aguilera CM, Mesa MD, Gil A. Omega-3 longchain polyunsaturated fatty acids supplementation on inflammatory biomakers: asystematic review of randomised clinical trials. Br J Nutr. 2012 Jun;107Suppl2:S159-70.
Roulet M, Frascarolo P, Pilet M, Chapuis G. Effects of intravenously infused fish oil on platelet fatty acid phospholipid composition and on platelet function in postoperative trauma. JPEN J Parenter Enteral Nutr. 1997 Sep-Oct;21(5):296-301.
Schrepf R, Limmert T, Claus Weber P, Theisen K, Sellmayer A. Immediate effects of n-3 fatty acid infusion on the induction of sustained ventricular tachycardia. Lancet. 2004 May 1;363(9419):1441-2.
Simoens CM, Deckelbaum RJ, Massaut JJ, Carpentier YA. Inclusion of 10% fish oil in mixed medium-chain triacylglycerol-long-chain triacylglycerol emulsions increases plasma triacylglycerol clearance and induces rapid eicosapentaenoic acid (20:5n-3) incorporation into blood cell phospholipids. Am J ClinNutr. 2008 Aug;88(2):282-8.
Snydman DR, Murray SA, Kornfeld SJ, Majka JA, Ellis CA. Total parenteral nutrition-related infections. Prospective epidemiologic study using semiquantitative methods. Am J Med. 1982 Nov;73(5):695-9. -Omega-6 is not mentioned anywhere in this article
Sungurtekin H, Değirmenci S, Sungurtekin U, Oguz BE, Sabir N, Kaptanoglu B. Comparison of the effects of different intravenous fat emulsions in patients with systemic inflammatory response syndrome and sepsis. NutrClinPract. 2011 Dec;26(6):665-71.
Tappy L, Berger MM, Schwarz JM, Schneiter P, Kim S, Revelly JP, Chioléro R. Metabolic effects of parenteral nutrition enriched with n-3 polyunsaturated fatty acids in critically ill patients.ClinNutr. 2006 Aug;25(4):588-95.
Tomsits E, Pataki M, Tölgyesi A, Fekete G, Rischak K, Szollár L. Safety and efficacy of a lipid emulsion containing a mixture of soybean oil, medium-chain triglycerides, olive oil, and fish oil: a randomised, double-blind clinical trial in premature infants requiring parenteral nutrition. J PediatrGastroenterolNutr. 2010 Oct;51(4):514-21.
Wei C, Hua J, Bin C, Klassen K. Impact of lipid emulsion containing fish oil on outcomes of surgical patients: systematic review of randomized controlled trials from Europe and Asia. Nutrition. 2010 May;26(5):474-81.
Wichmann MW, Thul P, Czarnetzki HD, Morlion BJ, Kemen M, Jauch KW. Evaluation of clinical safety and beneficial effects of a fish oil containing lipid emulsion (Lipoplus, MLF541): data from a prospective, randomized, multicenter trial. Crit Care Med. 2007 Mar;35(3):700-6.
Xiong J, Zhu S, Zhou Y, Wu H, Wang C. Regulation of omega-3 fish oil emulsion on the SIRS during the initial stage of severe acute pancreatitis. J HuazhongUnivSciTechnolog Med Sci. 2009 Feb;29(1):35-8.
Fish oil supplementation in early infancy modulates immune responses

This double-blind, randomized controlled trial examined the effect of early postnatal fish oil supplementation on infant cellular immune function at six months of age in the context of allergic disease (N = 420). Infants with high atopic risk received fish oil [280 mg docosahexaenoic acid (DHA) and 110 mg eicosapentanoic acid (EPA)] or control oil daily from birth to six months. Blood was collected and analyzed at six months of age in 120 infants and infant allergies were assessed at six and 12 months of age. DHA and EPA levels were significantly higher and erythrocyte arachidonic acid (AA) levels were lower in the fish oil group (all P < 0.05). Infants in the fish oil group had significantly lower IL-13 responses (P = 0.036) to house dust mite and higher IFNγ (P = 0.035) and TNF (P = 0.017) responses to phytohaemaglutinin. Infants with relatively high DHA levels had lower Th2 responses to allergens including lower IL-13 and IL-5 to β-lactoglobulin (P = 0.020 and P = 0.045, respectively). These results suggest that omega-3 fatty acids have immunomodulatory properties (lowered allergen-specific Th2 responses and elevated polyclonal Th1 responses) that are potentially allergyprotective. Clin Exp Allergy. 2012 Aug;42(8):1206-16. PMID: 22805468
Caffeine improves motor measures in patients with Parkinson disease

Epidemiologic studies consistently link caffeine, a nonselective adenosine antagonist, to lower risk of Parkinson disease (PD). This six-week randomized, placebo-controlled trial was conducted to assess the effects of caffeine (100 mg twice daily for three weeks and then 200 mg twice daily for three weeks) upon daytime somnolence, motor severity, and other nonmotor features in 61 PD patients with daytime somnolence. Caffeine resulted in a non-significant reduction in Epworth Sleepiness Scale score (-1.71 points; 95% CI -3.57 to 0.13). However, somnolence improved on the Clinical Global Impression of Change (+0.64; 95% CI 0.16-1.13), with significant reduction in Epworth Sleepiness Scale score on per-protocol analysis (-1.97; 95% CI -3.87 to -0.05). Caffeine reduced the total Unified Parkinson’s Disease Rating Scale score (-4.69 points; 95% CI -7.7 to -1.6) and the objective motor component (-3.15 points; 95% CI -5.50 to -0.83). Modest improvement in global health measures were found but no changes in quality of life, depression, or sleep quality were noted. The authors concluded that caffeine provided only equivocal borderline improvement in excessive somnolence in PD, but improved objective motor measures. These potential motor benefits suggest that a larger long-term trial of caffeine is warranted. Neurology. 2012 Aug 1. PMID: 22855866
Lactobacillus reuteri DSM 17938 effectively treats acute diarrhea in children

Probiotics seem to be efficacious for the management of acute diarrhea but the effect is strain specific. This randomized, double-blind trial was conducted to investigate the efficacy and safety of Lactobacillus reuteri DSM 17938 derived from L. reuteri ATCC 55730 (dose of 4 × 10(8) colony-forming units/die) in children with acute diarrhea. Subjects included children (6-36 months; N = 69) who had been hospitalized with acute diarrhea and had clinical signs of dehydration. Lactobacillus reuteri significantly reduced the duration of watery diarrhea compared to placebo (2.1 ± 1.7 days vs. 3.3 ± 2.1 days; P < 0.03). On day two and three of treatment, watery diarrhea persisted in 82% and 74% of the placebo group, and 55% and 45% of the treatment group, respectively (P < 0.01; P < 0.03). Finally, the L. reuteri group had a significantly lower relapse rate of diarrhea (15% vs. 42%; P < 0.03) although no significant differences in hospital stay were noted between the groups. This study revealed that L . reuteri DSM 17938 as an adjunct to rehydration therapy is efficacious and safe in the treatment of acute diarrhea. Aliment Pharmacol Ther. 2012 Aug;36(4):363-9. PMID: 22680836





