






This study was conducted to investigate the association of high sensitivity c-reactive protein (hsCRP) on early carotid atherosclerosis progression in a large, population-based cohort study. The study cohort included 839 young adults (aged 24 to 43 years, 70% white, 42% men) enrolled in the Bogalusa Heart Study, who underwent baseline examinations in 2001-2002 for measurements of cardiovascular disease risk factors. Progression of carotid artery intima-media thickness (IMT) was assessed during a mean follow-up of 2.4 years. Carotid artery IMT progression rates were as follows: composite carotid artery = 9.2 +/- 52 um/y, common carotid artery = 0.0 +/- 51 um/y, carotid bulb = 8.8 +/- 103 um/y, and internal carotid artery = 18.9 +/- 81 um/y. Elevated baseline hsCRP revealed an independent association with composite carotid artery IMT progression. Increased age, systolic blood pressure, fasting glucose, LDL cholesterol, and current smoking were also found to increase risk of carotid artery IMT progression in young adults. The authors concluded that this study underlines the importance of assesssing hsCRP levels along with smoking and traditional cardiovascular disease risk factor profiles in asymptomatic young adults. BMC Cardiovasc Disord. 2011 Dec 30;11(1):78. PMID: 22208681
Plasma antioxidant capacity is reduced in Asperger syndrome

Recent evidence suggests that children with autism may have an impaired detoxification capacity and suffer from chronic oxidative stress; however, the oxidative metabolism specifically in Asperger syndrome has not been studied. The current study investigated the oxidative status of a group of adolescent patients with Asperger syndrome, a group of adolescents with a first episode of psychosis, and a group of healthy controls. Total antioxidant status (TAOS), non-enzymatic (glutathione and homocysteine) and enzymatic (catalase, superoxide dismutase, and glutathione peroxidase) antioxidants, and lipid peroxidation were measured in plasma or erythrocyte lysates at baseline, 8 to 12 weeks, and one year. TAOS was found to be reduced in Asperger individuals compared with healthy controls and psychosis patients after covarying by age and antipsychotic treatment. This reduced antioxidant capacity did not depend on any of the individual antioxidant variables measured. Psychosis patients had increased homocysteine levels in plasma and decreased copper and ceruloplasmin at baseline. No impaired detoxifying capacity was found in the first year of illness in the group of adolescents with a first episode of psychosis. The authors concluded that Asperger patients seem to have a chronic low detoxifying capacity. J Psychiatr Res. 2012 Jan 4. PMID: 22225920
A vegan or vegetarian diet substantially alters the human colonic fecal microbiota

The influence of regular diets on intestinal microbiota is widely unknown. The current study examined fecal samples of vegetarians (n=144), vegans (n=105), and an equal number of control subjects consuming an omnivorous diet who were matched for age and gender. Classical bacteriological isolation was utilized and the main aerobic and anaerobic bacterial genera were identified and enumerated. Absolute and relative numbers were computed and compared between groups. Total counts of Bacteroides spp., Bifidobacterium spp., Escherichia coli and Enterobacteriaceae spp. were significantly lower (P=0.001, P=0.002, P=0.006 and P=0.008, respectively) in vegan samples than in controls, whereas others (E. coli biovars, Klebsiella spp., Enterobacter spp., other Enterobacteriaceae, Enterococcus spp., Lactobacillus spp., Citrobacter spp. and Clostridium spp.) were not. The total microbial count did not differ between the groups. In addition, subjects on a vegan or vegetarian diet showed significantly (P=0.0001) lower stool pH than did controls and stool pH and counts of E. coli and Enterobacteriaceae were significantly correlated across all subgroups. The authors concluded that maintaining a vegan or vegetarian diet results in a significant shift in the microbiota while total cell numbers remain unaltered. Eur J Clin Nutr. 2012 Jan;66(1):53-60. PMID: 21811294
Saturated Fat

Saturated Fat
Friend, foe, or simply neutral?
Abstract
There is widespread belief that saturated fat (SF) is adversely associated with coronary heart disease (CHD) and cardiovascular disease (CVD). This hypothesis has been incorporated into practice and nutritional guidelines. Specific targets for maximum amounts of SF as a percentage of dietary energy are also a common aspect of guidelines. Historically total fat was viewed as the culprit, but when evidence was not forthcoming, the focus shifted to SF. Central to this subject is the syllogism, i.e. SF elevates LDL cholesterol, LDL cholesterol causes heart disease and therefore SF causes heart disease. This syllogism falls apart when one examines its two critical components. First, there is a remarkably poor correlation between SF intake and LDL cholesterol, especially in the range of low intake to that common in North America. As regards the second component of the syllogism, LDL cholesterol levels are not related to the prevalence of adult coronary atherosclerosis, independent of age, gender or ethnicity. For asymptomatic individuals, cholesterol
is not a significant CHD/CVD risk factor for women, the elderly, or men over about 50 years of age. For younger men, the association may be seriously confounded by issues associated with blood pressure reactivity and stress. Lowering LDL with statin drugs in asymptomatic individuals has a near negligible effect on acute event risk (approximately 1% absolute risk reduction) which may be due to pleiotropic effects, and no impact on mortality. Finally, the association between SF and CHD or CVD has come under intense attack in the past two years. The overall conclusion is that there is no significant evidence for concluding that dietary SF is associated with the risk of CHD or CVD. This conclusion was already evident in 1998 but ignored. In addition, many studies find that SF does not appear to be a risk factor for several common cancers, nor with the risk of type2 diabetes, and if there is a weak association with insulin resistance, it does not appear to carry over to type 2 diabetes risk.
The original suggestion that there was a connection between saturated fat (SF) consumption and the risk of coronary heart disease was made on the basis of ecological studies. Such studies are notoriously prone to pointing in the wrong direction. This was followed by the observation that it was possible to elevate cholesterol and LDL cholesterol by feeding individuals excess saturated fat. Thus the syllogism: SF raises LDL, LDL causes heart disease, and therefore SF causes heart disease. In a comment in 2001 on an article in the journal Science titled “The Soft Science of Dietary Fat” (Taubes 2001), Scott Grundy, a high profile academic advocate of the diet-cholesterol-heart disease hypothesis, stated that, contrary to Taubes’ critical view, SFs are the main dietary cause of coronary heart disease (CHD) (Grundy 2001). This is still the conventional wisdom today with a number of guidelines recommending low SF consumption, typically ≤ 7% of total energy intake, although as will be discussed, there are a growing number of sceptics and a remarkable lack of evidence.
Keeping SF intake low was part of the low-fat diet movement, which started some 30-40 years ago. With the backing of governments, professional nutritional and medical associations and the media, fat was demonized and there was a significant move to lower intake. Low-fat products appeared on the supermarket shelves in ever increasing numbers. The calorie deficit was, for most followers of the new path, made up by carbohydrates and the carbohydrates turned out to be mostly the rapidly digestible, high glycemic variety. It is now generally recognized that this mass hysteria over fat had unintended consequences. Excess carbohydrate stimulated excess insulin production and fat storage, obesity, insulin resistance and the risk of diabetes. It is also ironic that in order to avoid a minor elevation in LDL of debatable clinical significance, those following the low-fat philosophy raised their triglycerides and lowered their HDL, in fact to an extent that was vastly more risky than the danger attributed to the minor elevation in LDL.
It is also important to recognize that nutritional studies which address the question of the association between dietary fat and various disorders present fundamental difficulties. If one macronutrient is decreased, then either it must be replaced by another macronutrient to maintain the same energy intake or the decrease in energy intake must be taken into account as a confounder. Either way, two critical variables are changed simultaneously. If the intake of A is reduced and B increased and benefit is observed with regard to, for example, the incidence of heart disease, this does not prove that the decrease in A was responsible or that A is a risk factor. In addition, randomized interventional nutrition studies, which are relied upon to produce definitive guidance, are frequently accompanied by failure to achieve the desired intakes, have poor long-term adherence to the study plan and frequently there is a convergence of the control and the intervention groups toward a common diet leading to non-significant results.
Hypotheses survive until falsified (to paraphrase Karl Popper). One is reminded of the famous black swan example. The hypothesis that saturated fat causes heart disease is now coming under scrutiny due to a number of studies which appear to directly falsify it, followed by several new meta-analysis which simply add confirmation. Recent research will be reviewed in this article along with related issues such as the connection between saturated fat and other diseases. In fact, the so-called Great Fat Debate is heating up (Zelman 2011). A number of black swans have been sighted.

THE SYLLOGISM: QUESTIONS
Earlier articles by the author which have appeared in this publication (Ware 2011a, Ware 2011b) presented strong evidence that LDL is not a risk factor for the prevalence or progression of coronary atherosclerosis in either diabetics or non-diabetics, and is a weak or for many individuals a non-existent risk factor for acute cardiac events. Lowering LDL with drugs in asymptomatic individuals carries an absolute risk reduction of only around 1% for acute events and no impact on cardiac related mortality, and the number needed to treat to prevent one non-fatal event is about 100. This small impact may also be a pleiotropic effect and have no connection with lipid lowering. Thus, the above chain of reasoning that leads from SF to LDL elevation to heart disease risk appears seriously weakened for these reasons alone.
Critical to the case against SF is its alleged ability to elevate cholesterol and LDL to an extent that is clinically significant. Based on a meta-analysis of metabolic ward studies, when 10% of energy intake from saturated fat was replaced by carbohydrates while keeping calorie intake constant, there was a decrease in LDL by 0.36 mmol/L (14 mg/dL) (Clarke 1997). Another meta-analysis, where 1% of energy from carbohydrates was replaced by various individual saturated fats keeping the total energy intake constant, found changes in LDL that ranged from 0.05 to -0.004 mmol/L (1.9 to -0.16 mg/dL) (Mensink 2003). But using these numbers, even a 5% or 10% change in energy from SFs produces an LDL change that is of the same size as the normal variation of LDL levels in any given individual seen over short periods of time (Hegsted 1987). Furthermore, this ignores the huge individual variations. Thus one can question the clinical significance of these small changes. Furthermore, the above studies are inconsistent with more recent studies.
In a 2008 paper (Volek 2008), the authors present a scatter plot (Fig. 5) from a frequently cited paper used to support the claim that saturated fat intake increases serum cholesterol (Clarke 1997). If one examines just the part of the plot ranging from 5% to 25% saturated fat intake as a percentage of total energy, a range that encompasses the intake of a majority of North Americans who on average consume about 14% of energy as SF, the correlation between SF intake and cholesterol is almost impossible to see, and if one looks at the range from 15% to 7%, approximately the change recommended by the current guidelines, the scatter is so great that this decrease in SF intake appears equally likely to raise as to lower total cholesterol. Volek and coauthors conclude that total cholesterol is not a strong predictor and find it hard to consider the cited figure as evidence of substantial benefit for reducing SF across the board.
These results alone are enough to generate justified skepticism, but they are strongly reinforced by two recent studies which also addressed the question of correlation between SF intake and LDL levels and found no association (Mirmiran 2009, Wood 2011). Thus the syllogism presented above appears to have fatal flaws.
OBSERVATIONAL AND INTERVENTION STUDIES. SATURATED FAT AND CHD/CVD
Already in 1998 a lengthy and comprehensive systematic review appeared in the Journal of Clinical Epidemiology which examined the evidence for and against the hypothesis that SF intake was related to either CVD incidence or mortality (Ravnskov 1998). A very large number of ecological (population) studies, as well as cross-sectional (snapshot), case-control and cohort follow-up studies were examined. In addition autopsy studies that examined the relationship between saturated fat (animal fat) intake and the extent of atherosclerosis were reviewed. Ravnskov did not find any convincing evidence up to 1998 for the association. The overall picture that emerged was one of inconsistency with more studies falsifying the hpothesis than supporting it, even when studies of comparable quality were compared in detail.
In 2005 a 20-year update on the famous Nurses’ Health Study also looked at the association between dietary fat intake and CHD (Oh 2005). When the results of this prospective cohort study were corrected for confounding, there was no significant relation between the relative risk of coronary heart disease and saturated fat intake when the lowest vs. the highest quintile were compared. The same was true for total fat intake, but polyunsaturated fat was found to be significantly protective and trans fats significantly harmful. This study involved the analysis of data from a lengthy follow-up study of over 78,000 female nurses.
A recent meta-analysis of 21 prospective epidemiologic studies and a pooled analysis of 11 cohort studies have recently appeared which have fueled the SF-heart disease debate. The pooled analysis (Jakobsen 2009) examined the impact on coronary events or CHD-related mortality associated with the various combinations of substitution of monounsaturated fatty acids (MUFAs), polyunsaturated fatty acids (PUFAs) or carbohydrates in place of SF. PUFA substitution was found to decrease the risk of both endpoints whereas carbohydrates were found to significantly increase the risk for coronary events but not mortality. MUFA substitution for SF was not associated with CHD risk. There was no effect modification by gender or age.
The second study, a meta-analysis of prospective studies (Siri-Tarino 2010a) examined the relationship between SF and cardiovascular disease (CVD). It was found that there was no significant evidence for concluding that dietary SF is associated with increased risk of CHD or CVD. The researchers comment that more data are needed to elucidate the question of CVD risks being associated with specific nutrients used to replace SF. Some would be satisfied at this point with the picture that has emerged.
In the introduction of the meta-analysis of Siri-Tarino et al, the authors point out that there are only a limited number of randomized clinical intervention trials that have examined the issue of saturated fat and CVD or CHD. The results have been inconsistent with some showing benefit, others none. Those what showed beneficial effects associated with reducing saturated fat intake replaced it with PUFAs. These positive results could have been due to simply an increase in PUFAs. The pooling study discussed above supports this conjecture.
THE ASSOCIATION OF SATURATED FAT WITH OTHER DISORDERS
Cancer. Interest in the potential association between cancer and dietary fat in general and saturated fat in particular has extended over more than two decades. Interest has focused on breast, prostate and colorectal cancer. For breast cancer, two recent very large meta-analyses did not support a positive independent association with either total fat or animal fat (Alexander 2010, Turner 2011). Meta-analyses for colorectal cancer were also negative (Alexander 2009, Liu 2011). Prospective studies failed to find a consistent association between fat and prostate cancer, but the risks associated with saturated fat are unclear (Dennis 2004). Reduction of consumption of processed meat may in general decrease cancer risk. However, here the issue appears to be carcinogens rather than fat (Kushi 2002).
Diabetes and Insulin resistance.
In the Nurses’ Health Study, total, saturated and monounsaturated fat were not associated with the risk of type 2 diabetes. Furthermore, polyunsaturated fat was protective and trans-fats increased risk (Salmeron 2001). In the Health Professionals Follow-up, saturated fat was not associated with the risk of type 2 diabetes in men once the results were adjusted for BMI (van Dam 2002). As regards fat type and insulin resistance, if fat intake was high, no fat-type dependence was found. No changes in insulin resistance were found when fat composition was kept constant but total intake varied between 20% and 40% of energy. However, if fat intake is low there is some evidence that saturated fat may decrease insulin sensitivity, but this does not carry over to increased incidence of diabetes (Siri-Tarino 2010b).
Decades ago, the traditional diet for diabetics involved severe carbohydrate restriction. As the 20th century progressed this became less popular and then with the advent of the highly successful anti-fat campaign, diabetic patients were warned of the extreme dangers of substituting fat for carbohydrates. Dr. Robert Atkins was brought before a U.S. congressional committee to defend the accusation that by promoting a low-carbohydrate (and therefore elevated fat) diet, he was seriously endangering public health, an accusation proven false by a number of studies over the past decade. Today there are calls for a return to this traditional approach of treating type 2 diabetes, and the merits of carbohydrate restriction in the context of diabetes prevention and therapy have been pointed out repeatedly in the past few years (Accurso 2008, Volek 2005a, Volek 2005b, Volek 2008, Volek 2009). The success achieved by Richard K. Bernstein using carbohydrate restriction and carefully selected carbohydrates matched to the individual’s metabolism is now documented in several editions of his book Dr. Bernstein’s Diabetes Solution (Bernstein 2011). The HbA1c levels he achieves are vastly better than anything conventional medicine appears able to achieve, and this is accomplished with diet. Drugs or insulin are used only when absolutely necessary. Taken together, the journal literature and the evidence in this book should give cause for reflection among diabetologists.
CONCLUSIONS
The fat-is-bad notion is alive and well as evidenced by the recent move by Denmark to place a special tax, thought to be the world’s first ever, on foods high in saturated fat. Health authorities in Denmark claim it will save countless lives. The scientists advising the government presumably refused to give any weight to the contrary evidence, in fact the lack of evidence, in the literature and the associated numerous commentaries, and in addition, to studies regarding the danger of substituting high glycemic index carbohydrates for fat. Yet the natural human tendency is to do just that and in particular to increase refined carbohydrates. The saturated fat saga is an excellent example of the tendency among professionals to ignore vast amounts of literature that disagree with their long-held beliefs. Hypotheses that appear to have been conclusively falsified have a remarkably long lifetime and vitality.
A reasonable approach to the dietary fat issue is perhaps simply to avoid all trans-fats (Aronis 2011), severely limit processed meats (Micha 2010), make sure of an adequate intake of omega-3 fatty acids and in particular, the long-chain fatty acids found in fish (Mozaffarian 2007), use general calorie restriction rather than specific macronutrient restriction when trying to lose weight and consider carbohydrate restriction when attempting to control blood sugar levels (Feinman 2008, Omodei 2011).
References
Accurso,A., Bernstein,R.K., Dahlqvist,A., Draznin,B., Feinman,R.D., Fine,E.J., Gleed,A., Jacobs,D.B., Larson,G., Lustig,R.H., Manninen,A.H., McFarlane,S.I., Morrison,K., Nielsen,J.V., Ravnskov,U., Roth,K.S., Silvestre,R., Sowers,J.R., Sundberg,R., Volek,J.S., Westman,E.C., Wood,R.J., Wortman,J. and Vernon,M.C. Dietary carbohydrate restriction in type 2 diabetes mellitus and metabolic syndrome: time for a critical appraisal. Nutr Metab (Lond) 2008; 5: 9.
Alexander,D.D., Cushing,C.A., Lowe,K.A., Sceurman,B. and Roberts,M.A. Meta-analysis of animal fat or animal protein intake and colorectal cancer. Am J Clin Nutr 2009; 89(5): 1402-1409.
Alexander,D.D., Morimoto,L.M., Mink,P.J. and Lowe,K.A. Summary and meta-analysis of prospective studies of animal fat intake and breast cancer. Nutr Res Rev 2010; 23(1): 169-179.
Aronis,K.N., Joseph,R.J., Blackburn,G.L. and Mantzoros,C. trans-Fatty acids, insulin resistance/diabetes, and cardiovascular disease risk: should policy decisions be based on observational cohort studies, or should we be waiting for results from randomized placebo-controlled trials? Metabolism 2011; 60(7): 901-905.
Bernstein,R.K., 2011. Dr Bernstein’s Diabetes Solution. The complete guide to acheiving normal blood sugars. Little, Brown and Company, New York.
Clarke,R., Frost,C., Collins,R., Appleby,P. and Peto,R. Dietary lipids and blood cholesterol: quantitative meta-analysis of metabolic ward studies. BMJ 1997; 314(7074): 112-117.
Dennis,L.K., Snetselaar,L.G., Smith,B.J., Stewart,R.E. and Robbins,M.E. Problems with the assessment of dietary fat in prostate cancer studies. Am J Epidemiol 2004; 160(5): 436-444.
Feinman,R.D. and Volek,J.S. Carbohydrate restriction as the default treatment for type 2 diabetes and metabolic syndrome. Scand Cardiovasc. J 2008; 42(4): 256-263.
Grundy,S.M. Dietary fat: at the heart of the matter. Science 2001; 293(5531): 801-804.
Hegsted,D.M. and Nicolosi,R.J. Individual variation in serum cholesterol levels. Proc Natl Acad Sci U. S. A 1987; 84(17): 6259-6261.
Jakobsen,M.U., O’Reilly,E.J., Heitmann,B.L., Pereira,M.A., Balter,K., Fraser,G.E., Goldbourt,U., Hallmans,G., Knekt,P., Liu,S., Pietinen,P., Spiegelman,D., Stevens,J., Virtamo,J., Willett,W.C. and Ascherio,A. Major types of dietary fat and risk of coronary heart disease: a pooled analysis of 11 cohort studies. Am J Clin Nutr 2009; 89(5): 1425-1432.
Kushi,L. and Giovannucci,E. Dietary fat and cancer. Am J Med 2002; 113 Suppl 9B: 63S-70S.
Liu,L., Zhuang,W., Wang,R.Q., Mukherjee,R., Xiao,S.M., Chen,Z., Wu,X.T., Zhou,Y. and Zhang,H.Y. Is dietary fat associated with the risk of colorectal cancer? A meta-analysis of 13 prospective cohort studies. Eur J Nutr 2011; 50(3): 173-184.
Mensink,R.P., Zock,P.L., Kester,A.D. and Katan,M.B. Effects of dietary fatty acids and carbohydrates on the ratio of serum total to HDL cholesterol and on serum lipids and apolipoproteins: a meta-analysis of 60 controlled trials. Am J Clin Nutr 2003; 77(5): 1146-1155.
Micha,R., Wallace,S.K. and Mozaffarian,D. Red and Processed Meat Consumption and Risk of Incident Coronary Heart Disease, Stroke, and Diabetes Mellitus. Circulation 2010; 121(21): 2271-2283.
Mirmiran,P., Ramezankhani,A. and Azizi,F. Combined effects of saturated fat and cholesterol intakes on serum lipids: Tehran Lipid and Glucose Study. Nutrition 2009; 25(5): 526-531.
Mozaffarian,D. JELIS, fishoil, and cardiac events. Lancet. 2007; 369(9567): 1062-3.
Oh,K., Hu,F.B., Manson,J.E., Stampfer,M.J. and Willett,W.C. Dietary fat intake and risk of coronary heart disease in women: 20 years of follow-up of the nurses’ health study. Am J Epidemiol 2005; 161(7): 672-679.
Omodei,D. and Fontana,L. Calorie restriction and prevention of age-associated chronic disease. FEBS Lett 2011; 585(11): 1537-1542.
Ravnskov,U. The questionable role of saturated and polyunsaturated fatty acids in cardiovascular disease. J Clin Epidemiol 1998; 51(6): 443-460.
Salmeron,J., Hu,F.B., Manson,J.E., Stampfer,M.J., Colditz,G.A., Rimm,E.B. and Willett,W.C. Dietary fat intake and risk of type 2 diabetes in women. Am J Clin Nutr 2001; 73(6): 1019-1026.
Siri-Tarino,P.W., Sun,Q., Hu,F.B. and Krauss,R.M. Meta-analysis of prospective cohort studies evaluating the association of saturated fat with cardiovascular disease. Am J Clin Nutr 2010a; 91(3): 535-546.
Siri-Tarino,P.W., Sun,Q., Hu,F.B. and Krauss,R.M. Saturated fat, carbohydrate, and cardiovascular disease. The American Journal of Clinical Nutrition 2010b; 91(3): 502-509.
Taubes,G. Nutrition. The soft science of dietary fat. Science 2001; 291(5513): 2536-2545.
Turner,L.B. A meta-analysis of fat intake, reproduction, and breast cancer risk: an evolutionary perspective. Am J Hum Biol 2011; 23(5): 601-608.
van Dam,R.M., Willett,W.C., Rimm,E.B., Stampfer,M.J. and Hu,F.B. Dietary fat and meat intake in relation to risk of type 2 diabetes in men. Diabetes Care 2002; 25(3): 417-424.
Volek,J.S. and Feinman,R.D. Carbohydrate restriction improves the features of Metabolic Syndrome. Metabolic Syndrome may be defined by the response to carbohydrate restriction. Nutr Metab (Lond) 2005a; 2: 31.
Volek,J.S., Fernandez,M.L., Feinman,R.D. and Phinney,S.D. Dietary carbohydrate restriction induces a unique metabolic state positively affecting atherogenic dyslipidemia, fatty acid partitioning, and metabolic syndrome. Prog. Lipid Res 2008; 47(5): 307-318.
Volek,J.S. and Forsythe,C.E. The case for not restricting saturated fat on a low carbohydrate diet. Nutr Metab (Lond) 2005b; 2: 21.
Volek,J.S., Phinney,S.D., Forsythe,C.E., Quann,E.E., Wood,R.J., Puglisi,M.J., Kraemer,W.J., Bibus,D.M., Fernandez,M.L. and Feinman,R.D. Carbohydrate restriction has a more favorable impact on the metabolic syndrome than a low fat diet. Lipids 2009; 44(4): 297-309.
Ware, RW. Does cholesterol drive coronary atherosclerosis? A critical review of available evidence. Integrated Healthcare Practitioners. October 2011a.
Ware, RW. Statin prescription for patients with diabetes. Yeah or nay? Integrated Healthcare Practitioners. November/ December 2011b.
Wood,A.C., Kabagambe,E.K., Borecki,I.B., Tiwari,H.K., Ordovas,J.M. and Arnett,D.K. Dietary Carbohydrate Modifies the Inverse Association Between Saturated Fat Intake and Cholesterol on Very Low-Density Lipoproteins. Lipid Insights. 2011; 2011(4): 7-15.
Zelman,K. The great fat debate: a closer look at the controversy-questioning the validity of age-old dietary guidance. J Am Diet Assoc 2011; 111(5): 655-658.
Low Back Pain and Pelvic Girdle Pain in PREGNANCY

Low Back Pain and Pelvic Girdle Pain in PREGNANCY
Assessment and management
Abstract
Low back pain (LBP) and pelvic girdle pain (PGP) associated with pregnancy are common problems that may be under-reported and under-treated. ese conditions have a signi cant impact on activities of daily living and may lead to chronic pain postpartum. While the exact etiology of LBP and PGP in pregnancy is not known, a combination of traumatic, hormonal and biomechanical mechanisms likely contribute to decreased integrity and stability in the back/pelvis during pregnancy. LBP and PGP can be di erentiated based on the location of pain; speci c pain provocation testing can be useful in the diagnosis of PGP. Exercise and acupuncture have been shown to reduce pain, improve functional ability and decrease disability in those with LBP and PGP associated with pregnancy; there is also some evidence for the use of spinal manipulative therapy and pelvic belts.
Half to two-thirds of women experience pregnancy related low back pain (PLBP) and/or pregnancy related pelvic girdle pain (PPGP) (Skaggs 2007, Wu 2004) yet it often goes unreported and untreated, perhaps because there is an assumption that it is a “normal” part of pregnancy. A recent survey found that only 32% of women with PLBP reported their pain to their prenatal care giver and only 25% of prenatal care providers recommended treatment (Wang 2004).
PLBP and PPGP have been correlated with disturbances to daily activities such as standing for 30 minutes, sleep disturbances, and use of pain medication (Mens 1996, Skaggs 2007, Wang 2004). It is therefore important for primary care practitioners to be knowledgeable and able to recommend effective treatment options.
Assessment and Diagnosis
Typically, PLBP is concentrated in the lumbar spine region, whereas PPGP is concentrated between the posterior iliac crests and gluteal fold, particularly in the region of the sacroiliac joint; this can occur in conjunction with or separately from pain in the symphysis (Vleeming 2008). Women are more likely to experience PLBP and PPGP if they have a history of previous low back pain (LBP), history of PLBP and PPGP, and strenuous work (Wu 2004).
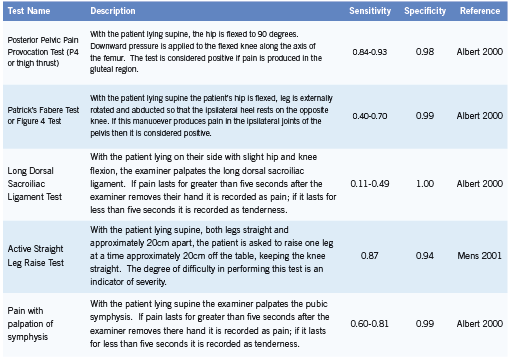
PPGP is diagnosed after other lumbar causes for the pain have been ruled out and when the pain is reproduced by specific clinical tests (Vleeming 2008). Pain provocation tests (Table 1) are useful in assessment and diagnosis of PPGP (Ronchetti 2008, Vleeming 2008).
Other serious causes of PLBP and PPGP must be ruled out with a thorough history and physical examination; differential diagnoses may include osteomyelitis, cauda equina syndrome, disc herniation, urinary tract infection, femoral vein thrombosis, or an obstetric complication.
Prognosis
Typically PPGP resolves within a few weeks to months after delivery but 8-10% of women continue to have pain for one to two years postpartum (Albert 2001, Rost 2006).While PLBP and PPGP are two separate clinical conditions, they can also occur in combination. Women who experience combined PLBP and PPGP appear more likely to experience LBP and pelvic girdle pain (PGP) during the post-partum period than those who experience just PLBP or PPGP (Gutke 2008, Turgut 1998). It is important to recognize that many non-pregnant women with chronic back pain identify pregnancy as the initial onset of their back pain (Mens 1996).
Etiology
The exact etiology of PLBP and PPGP is not clear and may in fact be multi-factorial.
Relaxin is a hormone that is produced in increased quantities during pregnancy and which leads to increased ligamentous laxity (MacLennan 1991).Women with PLBP and PPGP have been shown to have increased motion in their pelvic joints compared to healthy controls (Mens 2009). Smaller and flatter sacroiliac joints predicts an elevated risk of PLBP and PPGP; it has been hypothesized that as a result the loosening of the ligaments during pregnancy this joint becomes less stable (Vleeming 1990). Pain may result from increased shear forces across the sacroiliac joints.
Pregnancy also induces postural and biomechanical changes which could affect the stability of the lumbar spine and pelvis, thereby leading to pain. Increased abdominal muscle length (Fast 1990, Gilleard 1996) and altered angle of insertion have been noted for the rectus abdominus (RA) and have been correlated with the inability to stabilize the pelvis against resistance (Gilleard 1996). Studies using ultrasound have identified increased cross-sectional area of the RA and decreased RA thickness following delivery and in comparison to nulliparous controls (Coldron 2008, Weiss 2009). Sihvonen (1998) also found that changes to the functioning of back extensor muscles were related to back pain in pregnancy. It is possible that changes to the morphology of these muscles could reduce their ability to stabilize the spine and pelvis. Other contributing factors may include altered posture, muscle fatigue, muscle imbalance and previous trauma (Kristiansson 1996, Mens 1996, Perkins 1998).
Conservative Management Prevention
There is some evidence that exercise may play a role in preventing PLBP and PPGP (Mogren 2005, Mørkved 2007). A retrospective study by Mogren (2005) found that a higher number of years of regular leisure physical activity was associated with decreased risk of low back and pelvic pain during pregnancy (p=0.010).
A randomized control trial comparing a 12-week preventative exercise training program to usual care demonstrated positive results in a nulliparous pregnant population (Mørkved 2007). At 36 weeks gestation women in the training group were significantly less likely to report lumbopelvic pain (44% vs 56%; p=0.03) and had significantly higher scores of functional status on Disability Rating Index (DRI) (p=0.01) (Mørkved 2007).
Education
Education as a stand-alone strategy has received little focus for the management of PLBP and PPGP, however many studies include education as a component of a comprehensive program (Elden 2005, Mens 2000, Stuge 2004). Education on relevant anatomy and biomechanics, advice regarding ergonomics of daily activities and reassurance are commonly included and may help to reduce anxiety and fear in women with PLBP and PPGP (Vleeming 2008).
Exercise
In the non-pregnant population alterations to the functioning of the deep abdominal musculature play a role in LBP and exercise programs targeting these muscles appear effective in treating LBP (Ferreira 2010, Hides 2010). Since changes to morphology and functioning of both abdominal and low back musculature have been identified during pregnancy, it is reasonable to consider exercises which target the core musculature as a possible treatment during pregnancy.
Interventions including stabilizing exercises have been shown to be effective in reducing pain and improving functional ability in women with PLBP and PPGP (Elden 2005, Kluge 2011, Stuge 2004). Kluge (2011) compared pain intensity and functional ability in pregnant women before and after either specific stabilizing exercise program or control intervention. Pain intensity decreased in the intervention group from 30.0 to 18.5 (p<0.01); there was also a significant difference in pain intensity between the two groups following the intervention (18.5 compared to 33.0; p<0.01).
The sitting pelvic tilt exercise has been found to be an effective treatment in the third trimester (Suputtitada 2002). Compared to a control group, those performing the exercise had significantly lower pain intensities as measured by visual analogue scale (VAS) after 56 days of performing the exercise (p<0.05) (Suputtitada 2002).
Stuge (2004a) studied the role of exercise in treating PLBP and PPGP during the postpartum period. Physical therapy including ergonomics, massage, joint mobilization, manipulation, electrotherapy, and hot packs was compared to physical therapy plus exercises targeting the core musculature over a 20 week period. Exercise plus physical therapy resulted in statistically and clinically significant lower back pain intensity both in the morning (VAS; p=0.001) and evening (VAS; p<0.001) and lower disability as measured by Oswestry Disability Index (p<0.001) ) compared to those receiving physical therapy only. Differences between groups remained at one and two years postpartum (Stuge 2004b).
In a prospective trial pregnant women were randomized to watergymnastics or a control group; subjects in the water-gymnastics group participated in a once-weekly program for approximately 17-20 weeks. Significantly more women in the control group (17) versus water-gymnastics group (seven) were on sick-leave for back/ LBP after week 32-33 (p=0.031) (Kihlstrand 1999).
Overall exercise targeting the muscles that stabilize the back and pelvis and water gymnastics appear to be effective treatment options, however a few studies have found inconsistent results (Mens 2000, Nilsson-Wikmar 2005).
Spinal Manipulative Therapy
Spinal manipulative therapy (SMT) is an effective treatment for low back pain in the non-pregnant population (van Tulder 2006). While SMT may be effective for treating PLBP and PPGP, most studies in pregnant populations have combined SMT with other interventions such as exercise and myofascial release making it difficult to determine the effect of individual treatment modalities (Lisi 2006, Skaggs 2005, Stuge 2004).
For example, Skaggs (2005) applied a multimodal treatment protocol including education, soft tissue mobilization, joint mobilization and manipulation and specific stabilization exercise to 170 patients. Patients were evaluated on the first and second visit using the Bournemouth Questionnaire; the average score on the first visit was 45 (SD=23) and second visit was 34 (SD=22). The difference in scores indicated significant improvement (p<0.01).
Retrospective case series have demonstrated that pregnant women with PLBP who underwent chiropractic care (including SMT) had clinically important improvement on Numerical Rating Scale pain score (Lisi 2005) and reported relief (Diakow 1991).
Acupuncture
Elden (2005) found acupuncture to be superior to standard treatment including information, advice, pelvic belt, and home exercise program targeted to abdominal and gluteal muscles. Following six weeks of twice per week acupuncture, the acupuncture and standard treatment groups differed in pain intensity in the morning (p<0.001) and in the evening (p<0.001) as measured on VAS (Elden 2005). Similar results were also found by Kvorning (2004).
Guerreiro da Silva (2004) compared conventional treatment (pharmacotherapy: paracetamol and hyoscine) to conventional treatment plus acupuncture. Women in the acupuncture group showed a greater reduction in average pain on a numerical rating scale 0-10 (-4.8 points) compared to the control group (-0.3 points; p<0.0001). In addition, use of paracetamol decreased more in the acupuncture group (2.0) versus the control group (0.0; p=0.005).
Pelvic Belts
There is some evidence that pelvic belts help stabilize the pelvis and may be useful in the diagnosis and treatment of PLBP and PPGP. Mens et al (2002) found that pelvic belts significantly decreased sacroiliac joint laxity (p<0.001) and are more effective when positioned directly below the anterior superior iliac spine rather than at the level of symphysis pubis (p=0.006). Use of a pelvic belt has also been correlated with decreased score on the active straight leg test (Mens 2006). Another study by Carr (2003) found a lumbrosacral orthosis to be helpful in reducing pain intensity and effect of pain on daily activities during pregnancy. Pelvic belts are often used in combination with other interventions as part of a comprehensive treatment program.
Other
Other non-conservative treatment options may include pharmacotherapy, prolotherapy, surgery and injection therapy, but are beyond the scope of this paper.
Conclusion
PLBP and PPGP are common problems which significantly impact the activities of daily living in pregnant women. While the etiology is not clear, and may in fact be multi-factorial, the ability to stabilize the lumbar spine and pelvis appears compromised during pregnancy. Exercise and acupuncture are effective conservative treatment options; education, pelvic belts, and spinal manipulative therapy also appear to be useful. Health care providers working with this population should educate patients and consider recommending conservative treatment options.
References
Albert H, Godskesen M, Westergaard J. Prognosis in four syndromes of pregnancyrelated pelvic pain. Acta Obstet Gynecol Scand. 2001; 80: 505-511.
Albert H, Godskesen M, Westergaard J. Evaluation of clinical tests used in classification procedures in pregnancy-related pelvic joint pain. Eur Spine J. 2000; 9: 161-166.
Carr CA. Use of a maternity support binder for relief of pregnancy-related back pain. J Obstet Gynecol Neonatal Nurs.2003; 32: 495-502.
Coldron Y, Stokes M, Newham D, Cook K. Postpartum characteristics of rectus abdominus on ultrasound imaging. Manual Therapy.2008; 13: 112-121.
Diakow RP, Gadsby TA, Gadsby JB, Gleddie JG, Leprich DJ, Scales AM. Back pain during pregnancy and labor. J Manipulative PhysiolTher.1991; 14: 116-18.
Elden H, Ladfors L, Olsen M, Ostgaard H, Hagberg H. Effects of acupuncture and stabilizing exercises as adjunct to standard treatment in pregnancy women with pelvic girdle pain: randomised single blind controlled trial. BMJ.2005; 330: 761-766.
Fast A, Weiss L, Ducommun E, Medina E, Butler J. Low-back pain in pregnancy. Abdominal muscles, sit-up performance and back pain. Spine. 1990; 15(1): 28-30.
Ferriera P, Ferriera M, Maher C, Refshauge K, Herbert R, Hodges P. Changes in recruitment of transverses abdominis correlate with disability in people with chronic low back pain. Br J Sports Med. 2010; 44 (16): 1166-72.
Gilleard WL, Brown JMM. Structure and function of the abdominal muscles in primigravid subjects during pregnancy and the immediate postbirth period. Physical Therapy.1996; 76: 750-762.
Guerreiro da Salva JB, Nakamura MU, Cordeiro JA, Kulay L Jr. Acupuncture for low back pain in pregnancy- a prospective, quasi-randomised, controlled study. Acupunct Med. 2004; 22(2): 60-7.
Gutke, A, Ostgaard H, Oberg B. Predicting persistent pregnancy-related low back pain. Spine. 2008; 33: E386-E393.
Hides JA, Stanton WR, Wilson SJ, Freke M, MeMahon S, Sims K. Retraining motor control of abdominal muscles among elite cricketers with low back pain. Scand J Med Sci Sports. 2010; 20(6): 834-42.
Kihlstrand M, Stenman B, Nilsson S, Axelsson O. Water-gymnastics reduced the intensity of back/low back pain in pregnancy women. Acta Obstet Gynecol Scand.1999; 78: 180-185.
Kluge J, Hall D, Louw Q, Theron G, Grové D. Specific exercises to treat pregnancyrelated low back pain in a South African population. Int J Gynaecol Obstet. 2011; 113(3): 187-91.
Kristiansson P, Savardsudd K, von Schoultz B. Back pain during pregnancy. A prospective study. Spine.1996; 21: 1363-1370.
Kvorning N, Holmberg C, Grennert L, Aberg A, Akeson J. Acupuncture relieves pelvic and low-back pain in late pregnancy. Acta Obstet Gynecol Scand. 2004; 83(3): 246-50.
Lisi AJ. Chiropractic spinal manipulation for low back pain of pregnancy: a retrospective case series. J Midwifery Womens Health. 2006; 51: e7-e10.
MacLennan AH. The role of the hormone relaxin in human reproduction and pelvic girdle relaxation. Scand J Rheumatol Suppl. 1991; 88: 7-15.
Mens JMA, Pool-Goudzwaard A, Stam HJ. Mobility of the Pelvic Joints in Pregnancy-Related Lumbopelvic Pain. Obstet Gynecol Surv. 2009; 64: 200-208.
Mens JMA, Damen L, Snijders CJ, Stam HJ. The mechanical effect of a pelvic belt in patients with pregnancy-related pelvic pain. Clin Biomech. 2006; 21(2): 122-127.
Mens, JM, Vleeming A, Snijders CJ, Koes BW, Stam HJ. Reliability and validity of the active straight leg raise test in posterior pelvic pain since pregnancy. Spine. 2001; 26(10): 1167-71.
Mens JM, Snijders CJ, Stam HJ. Diagonal trunk muscle exercises in peripartum pelvic pain: a randomized clinical trial. Phys Ther. 2000; 80: 1164-1173.
Mens, JMA, Vleeming MB, Stoeckart T, Stan HJ, Snijders CJ. Understanding peripartum pelvic pain. Implications of a patient survey. Spine. 1996; 21: 1363-1370.
Mogren IM. Previous physical activity decreases the risk of low back pain and pelvic pain during pregnancy. Scand J Public Health. 2005; 33: 300-306.
Mørkved S, Salvesen KA, Schei B, Lydersen S, Bø K. Does group training during pregnancy prevent lumbopelvic pain? A randomized clinical trial. Acta Obstet Gynecol Scand. 2007; 86: 276-282.
Nilsson-Wikmar L, Holm K, Oijerstedt R, Harms-Ringdahl K. Effect of three different physical therapy treatments on pain and activity in pregnant women with pelvic girdle pain: a randomized clinical trial with 3, 6 and 12 months follow-up postpartum. Spine.2005; 30: 850-856.
Perkins J, Hammer R, Loubert P. Identification and management of pregnancyrelated low back pain. J Nurse Midwifery. 1998; 43(5): 331-339.
Ronchetti I, Vleeming A, van Wingerden J. Physical characteristics of women with severe pelvic girdle pain after pregnancy. A descriptive cohort study. Spine 2008. 33: E145-151.
Rost CC, Jacqueline J, Kaiser A, Verhagen AP, Koes BW. Prognosis of women with pelvic pain during pregnancy: a long-term follow-up study. Acta Ostet Gynecol Scand. 2006; 85: 771-777.
Sihvonen T, Huttunen M, Makkonen M, Airaksinen O. Functional Changes in Back Muscle Activity Correlate With Pain Intensity and Prediction of Low Back Pain During Pregnancy. Arch Phys Med Rehabil.1998; 79: 1210-2.
Skaggs C, Prather H, Gross G, George J, Thompson P, Nelson D. Back and pelvic pain in an underserved United States pregnancy population: A preliminary descriptive survey. J Manipulative PhysiolTher. 2007; 30: 130-134.
Skaggs CD, Gross G, Ducar D, Thompson PA, Nelson DM. A comprehensive musculoskeletal management program reduces pain and disability in pregnancy. J Chiropr Educ. 2005; 19: 31-2. (abstr)
Stuge B, Laerum E, Kirkesola G, Vøllestad N. The efficacy of a treatment program focusing on specific stabilizing exercises for pelvic girdle pain after pregnancy. Spine 2004a; 29: 351-359.
Stuge B, Veierød MB, Laerum E, Vøllestad N. The efficacy of a treatment program focusing on specific stabilizing exercises for pelvic girdle pain after pregnancy: a twoyear follow-up of a randomized clinical trial. Spine. 2004b; 29(10): E197-203.
Suputtitada A, Wacharapreechanont T, Chaisayan P. Effect of the “sitting pelvic tilt exercise” during the third trimester in primigravidas on back pain. J Med Assoc Thai. 2002; 85 Suppl 1: S170-9.
Turgut F, Turgut M, Cetinsahin M. A prospective study of persistent back pain after pregnancy. Eur J Obstet Gynecol Reprod Biol. 1998; 80: 45-48.
Vleeming A, Albert H, Östgaard HC, Sturesson B, Stuge B. European guidelines for the diagnosis and treatment of pelvic girdle pain. Eur Spine J. 2008; 17: 794-819.
Vleeming A, Stoeckart R, Volkers AC, Snijders CJ. Relation between form and function in the sacroiliac joint. Part I. Clinical anatomical aspects.Spine.1990; 15: 130-132.
Van Tulder R, Becker A, Bekkering T, Breen A, del Real MT, Hutchinson A, Koes B, Malmivaara A. European guidelines for the management of acute nonspecific low back pain in primary care. Eur Spine J. 2006; 15 Suppl 2: S169-91.
Wang SM, Dezinno P, Maranets I, Berman MR, Caldwell-Andrews AA, Kain ZN. Low back pain during pregnancy: prevalence, risk factors, and outcomes. Obstet Gynecol. 2004 Jul; 104(1): 65-70.
Weiss C, Triano J, Campbell M, Croy M. Abdominal muscle thickness in postpartum vs. nulliparous women: A preliminary study. J of Chiropr Educ. 2009; 23(1): 100. (abstr)
Wu H, Meijer O, Uegaki K, Mens J, van Dieen J, Wuisman P, Ostgaard H. Pregnancy-related pelvic girdle pain (PPP)I: Terminology, clinical presentation and prevalence. Eur Spine J. 2004; 13: 575-589.
Automated Breast Ultrasound (ABUS)

Automated Breast Ultrasound (ABUS)
Making Mammography Obsolete
Abstract There is a growing body of evidence that suggests the harms associated with standard breast cancer screening exams (mammography, breast self-examinations, and clinical breast exams) may outweigh the benefits. These harms include false-positive results, over-diagnosis, and over-treatment. Automated breast ultrasound (ABUS) is one of the latest technological breakthroughs that have been proposed as a suitable alternative for breast cancer screening. ABUS is a safe, painless, radiation-free, and non-invasive technology. It is a 3D ultrasound technology that is specifically developed for whole breast imaging and allows for images of high-resolution to be produced. Although somewhat limited, the currently available evidence is reviewed and appears to support the use of ABUS as a valuable screening tool, especially when considering the risks and benefits of the available alternatives. ABUS has also been studied in comparison to mammography, hand-held ultrasound, and MRI. In all studies, ABUS appears to provide additional value in terms of its sensitivity and specificity. ABUS appears to have high accuracy in determining preoperative cancer lesions and appears to be accurate in analyzing all types of histological subgroups. The main limitation in the studies that have been conducted is that they included a higher proportion of malignant lesions or breast masses than would be found in the screening population. Other limitations are that interpreting ABUS data requires a learning curve and that ABUS may be less valuable when it comes to examining the axillary regions or when examining the vascularity and elasticity of breast lesions. Largerscale research will need to be conducted on this exciting technology to determine its exact role in breast cancer screening, but ABUS will likely prove to be a cost-effective alternative.
In Canada, regular screening for breast cancer occurs with mammography, breast self-examinations, and clinical breast exams (Shields 2009). Currently, there exists controversy over exactly which screening tools should be utilized for particular patient populations. These three screening exams are recommended to reduce mortality due to breast cancer, but there is a growing body of evidence that suggests that the harms associated with these exams may outweigh the benefits (Canadian Task Force 2011). These harms include false-positive results, over-diagnosis, and over-treatment. In addition, positive results often cause emotional pain and anxiety for patients that can be severe and have long-term implications (Montgomery 2010). As such, there is a high demand for an alternative that reduces these harms and yet provides clinically useful information.
Automated breast ultrasound (ABUS) is one of the latest technological breakthroughs that have been proposed as a suitable alternative for breast cancer screening (Wenkel 2008). ABUS is a safe, painless, radiation-free, and non-invasive technology. It is a 3D ultrasound technology that is specifically developed for whole breast imaging and allows for images of high-resolution to be produced (Lin 2011). It has also been referred to in the literature as automated breast volume scanning (ABVS), automated whole-breast ultrasound (AWBS), and sonographic tomography (Kelly 2010). In this article, it will only be referred to as ABUS for simplicity. Although somewhat limited, the currently available evidence appears to support the use of ABUS as a valuable screening tool, especially when considering the risks and benefits of the available alternatives. This article will review the studies that have been conducted and discuss the value of ABUS compared to other breast imaging methods.
A recent pilot study of ABUS was conducted to evaluate its ability to detect and classify breast lesions according to the Breast Imaging Reporting and Data System (BI-RADS) (Wenkel 2008). Thirty-five women who had unclear findings in breast diagnosis performed through palpation, sonography, or mammography were selected and received ABUS. Five radiologists independently evaluated the ABUS images and classified them according to BI-RADS. All breast cancers were found with the ABUS by all examiners and correctly classified in the BI-RADS. In this study, ABUS allowed detection of solid and cystic lesions and their BI-RADS classification with a high reliability. This study was not without limitations. The first limitation was that the selected patient group had a high number of lesions and thus did not reflect a screening population. Another limitation was that some histological subgroups such as medullary carcinoma and ductal carcinoma in situ were not present in the cohort and thus the researchers could not comment on the ability of ABUS to detect these subgroups. Finally, only the affected breast was scanned and analyzed, possibly resulting in a high degree of alertness by the radiologists.
Another recent study of ABUS was conducted to determine the accuracy of measuring preoperative cancer extent (Tozaki 2010). This retrospective study looked at forty patients with histopathologically confirmed breast cancer who underwent ABUS on the day prior to surgery. The age range of patients was 31-76 years old. The discrepancy of the tumor extent between ABUS and the histological examination was calculated. It was found that ABUS enabled visualization of the breast carcinomas in all patients. The histopathological diagnosis was ductal carcinoma in situ in seven patients and invasive ductal carcinoma in thirty-three patients. The accuracy of determination of the tumor extent with a deviation in length of less than 2cm was 98%. This particular study helps fill gaps in the evidence to support the use of ABUS for these particular histological subgroups.
The same researchers have also studied the optimal scanning technique to cover the whole breast using ABUS (Tozaki 2010). In this study, forty patients aged 23-68 years old underwent ABUS in the upper-outer, lower-outer, lower-inner, and upperinner breast regions. Three examiners were used. The researchers also compared ABUS to hand-held ultrasound (HHUS). In total, sixty-one lesions were detected by HHUS and this number was consistent with those found by ABUS. No comment could be made when comparing the diagnostic accuracy of ABUS due to the small number of histologically confirmed lesions. The total scanning time for ABUS ranged from 10-12 minutes, which is fairly reasonable. All four scanning techniques for the major segments of the breast were found to be operator-independent and feasible for performing ABUS. Some of the disadvantages for ABUS that were identified by this study included the difficulty in examining the axillary regions, as well as analyzing the vascularity and elasticity of the breast lesions. Overall, this study indicates that ABUS is comparable to HHUS with regards to scanning technique, but with the additional benefit of being operator-independent.
Breast cancer detection using mammography plus ABUS compared to mammography alone has been studied (Kelly 2010). Twelve radiologists were blinded and provided with images of radiographically dense breasts. Half of the images were malignant. The radiologists first reviewed the mammograms and assessed their likelihood ratings based on BI-RADS and the Digital Mammographic Imaging Screenings Trial (DMIST). The radiologists then reviewed the mammograms with the ABUS data. Performance across screening techniques was compared using absolute callback, areas under the curve, and with figure of merit. With ABUS, true positives of cancer detection increased by 63% with only a 4% decrease in true negatives. The area under the curve average and the figure of merit were higher when mammography was paired with ABUS compared to mammography alone. Therefore, this study concluded that for dense-breasted women, incorporating ABUS with mammography adds significant clinical value. The automated process for breast ultrasound eliminates operator variability, provides greater consistency, and ensures reproducibility of quality images. Similar to one of the studies that were discussed previously, one limitation of this study might have been that the radiologists could have been extremely vigilant by realizing that the test images had higher rates of lesions than in a normal population.
ABUS has also been compared to MRI in a retrospective analysis (Grady 2010). Forty-one women who were diagnosed with breast cancer had preoperative staging using ABUS. They subsequently underwent bilateral contrast-enhanced MRI prior to surgery to determine tumor extension and other information regarding the spread of the cancer. Both imaging techniques were compared for accuracy to pathologic truth. ABUS accurately staged breast cancer preoperatively in 68% of cases, while MRI only did so in 54% of cases. ABUS resulted in an overall improvement in accuracy of 14% and thus appears superior to contrast-enhanced bilateral breast MRI. A second more recent study has also compared ABUS to MRI and determined how closely their results match (Moon 2011). ABUS and MRI breast images were obtained from forty patients; bilaterally in twenty-seven patients and unilaterally in thirteen patients. Calculated values for percent density and breast volume were compared and found to be highly correlated. These studies together appear to support ABUS as being equal to or superior to MRI.
The diagnostic accuracy of ABUS, including its sensitivity and specificity has been studied (Wojcinski 2011). In one study, ABUS data sets from fifty patients were collected and a database was created containing twenty-three women who had no detectable lesions with conventional ultrasound, thirteen women with benign lesions, and fourteen women with known breast cancer. An independent examiner evaluated the ABUS data on a separate workstation without any prior knowledge of the patients. The diagnostic accuracy for the ABUS was 66.0%. All breast cancers were detected, resulting in a sensitivity of 100%.
However, due to the high number of requests for second-look ultrasounds, specificity was 52.8%. In this study, the researchers concluded that ABUS must still be regarded as an experimental technique. The main limitations identified in this study were that the design had a limited sample size and that the proportion of cases to controls was not representative of the whole population.
The difference between ABUS and HHUS in detecting and diagnosing breast lesions has been examined and has provided further data on its diagnostic value (Lin 2011). In this study, eighty-one patients were subjected to both examinations and the number of lesions detected was compared. Diagnostic accuracy and specificity were calculated. Ninety-five lesions were detected by both devices. Both exhibited a sensitivity of 100% and a high specificity (ABUS 95.0% and HHUS 85.0%). ABUS had a higher diagnostic accuracy (97.1%) than HHUS (91.4%) for breast neoplasms. ABUS was also capable of displaying the retraction phenomenon in coronal plane, which produced a high specificity (100.0%) and a high sensitivity (80.0%) in detecting breast cancer, while it also had a high accuracy (91.4%) in determining malignant from benign lesions. A second study also looked at the differences between ABUS and HHUS (Isobe 2011). Sixty patients underwent ABUS and HHUS and four segments were scanned. In fourteen of the fifteen patients with breast lesions under the nipple, the lesions were detectable with both HHUS and ABUS. In the other patient, the lesion was not detectable by HHUS but was detected by ABUS. Overall, these two studies show that ABUS likely has superior diagnostic accuracy when compared to HHUS.
The inter-observer agreement of radiologists looking at breast masses that were detected by ABUS has been evaluated (Zhang 2011). In this study, 208 patients were subjected to ABUS and data were automatically sent to the ABUS workstation. Two radiologists evaluated 234 breast masses (148 benign and 86 malignant). The reviewers were blinded to the patient’s mammographic images, medical history, and pathologic findings. Substantial agreement was obtained for lesion shape, orientation, margin, echo pattern, posterior acoustic features, calcification, and final assessment. Fair agreement was obtained for retraction phenomenon and lesion boundary. This study provides evidence that inter-observer agreement for ABUS is high.
Researchers have retrospectively evaluated the detection of benign and malignant breast masses using ABUS data to determine which lesion variables affect detectability (Chang 2011). In this study, bilateral whole breast images were obtained using ABUS in sixtyseven consecutive women who were scheduled to undergo needle biopsy due to suspicious breast masses. Twenty-four invasive ductal cancers in twenty-three breasts, forty-six benign breast lesions in forty-four breasts, and thirty-eight normal breasts were included. Three breast radiologists who did not perform the examinations and were blinded to the histology reviewed the ABUS data. Sensitivities for benign mass detection ranged from 56.3% to 66.7% and for malignant masses ranged from 87.5% to 95.8%, indicating significantly higher sensitivity for malignant breast masses. The overall specificity was 79.5%. An analysis showed that mass size, surrounding tissue changes, and shape of the mass were the variables associated with detectability at ABUS. The lower detection rate for benign lesions was attributed to the fact that they only included solid breast lesions and not cystic lesions, which are easier to detect. This study was limited by the patient group that had a high number of lesions and did not represent a screening population. There also exists a learning curve in interpreting ABUS and these particular radiologists had little prior experience with ABUS, which may have affected the results.
In terms of financial cost, ABUS will probably prove cost-effective as a supplement to mammography for women with dense breasts (Feig 2010). Once radiologists have had practice with interpreting ABUS data and have progressed along the learning curve, it is likely that ABUS will provide clinicians with valuable diagnostic information. The ABUS system has an excellent safety profile and it is painless, radiation-free, and non-invasive. The evidence available demonstrates that it is specifically developed for whole breast imaging, but that it may be less valuable when it comes to examining the axillary regions or when examining the vascularity and elasticity of breast lesions. Some of the other variables that may limit its ability to detect breast lesions also include mass size and shape as well as surrounding tissue changes. Even so, ABUS appears to have high accuracy in determining preoperative cancer lesions and appears to be accurate in analyzing all types of histological subgroups. The evidence available seems to suggest that ABUS performs better than mammography, MRI, and HHUS and that inter-rater agreement for ABUS data are high. Its sensitivity and specificity are both high, especially when comparing these values to those of alternative screening methods. Many of the studies that have been done included a higher proportion of malignant lesions or breast masses than would be found in the screening population, meaning that it is likely too early to recommend ABUS as an independent screening tool. Larger-scale research will need to be conducted on this exciting technology to determine its exact role in breast cancer screening.
References
Canadian Task Force on Preventive Health Care, Tonelli M, Gorber SC, Joffres M, Dickinson J, Singh H, Lewin G, Birtwhistle R, Fitzpatrick-Lewis D, Hodgson N, Ciliska D, Gauld M, Liu YY. Recommendations on screening for breast cancer in average-risk women aged 40-74 years. CMAJ. 2011;183(17):1991-2001.
Chang JM, Moon WK, Cho N, Park JS, Kim SJ. Radiologists’ performance in the detection of benign and malignant masses with 3D automated breast ultrasound (ABUS). Eur J Radiol. 2011;78(1):99-103.
Feig S. Cost-effectiveness of mammography, MRI, and ultrasonography for breast cancer screening. Radiol Clin North Am. 2010;48(5):879-91.
Grady I, Gorsuch-Rafferty H, Hansen P. Sonographic tomography for the preoperative staging of breast cancer prior to surgery. Journal of Ultrasound. 2010;13(2):41-45.
Isobe S, Tozaki M, Yamaguchi M, Ogawa Y, Homma K, Satomi R, Saito M, Joo C, Fukuma E. Detectability of breast lesions under the nipple using an automated breast volume scanner: comparison with handheld ultrasonography. Jpn J Radiol. 2011;29(5):361-5.
Kelly KM, Dean J, Lee SJ, Comulada WS. Breast cancer detection: radiologists’ performance using mammography with and without automated whole-breast ultrasound. Eur Radiol. 2010;20(11):2557-64.
Lin X, Wang J, Han F, Fu J, Li A. Analysis of eighty-one cases with breast lesions using automated breast volume scanner and comparison with handheld ultrasound. Eur J Radiol. 2011. doi:10.1016/j.ejrad.2011.02.038
Montgomery M and McCrone SH. Psychological distress associated with the diagnostic phase for suspected breast cancer: systematic review. Journal of Advanced Nursing. 2010; 66(11), 2372–2390.
Moon WK, Shen YW, Huang CS, Luo SC, Kuzucan A, Chen JH, Chang RF. Comparative study of density analysis using automated whole breast ultrasound and MRI. Med Phys. 2011;38(1):382-9.
Shields M, Wilkins K. An update on mammography use in Canada. Health Rep. 2009;20(3):7-19.
Tozaki M, Fukuma E. Accuracy of determining preoperative cancer extent measured by automated breast ultrasonography. Jpn J Radiol. 2010;28(10):771-3.
Tozaki M, Isobe S, Yamaquchi M, Ogawa Y, Kohara M, Joo C, Fukama E. Optimal scanning technique to cover the whole breast using an automated breast volume scanner. Jpn J Radiol. 2010;28(4):325-8.
Wenkel E, Heckmann M, Heinrich M, Schwab SA, Uder M, Schulz-Wendtland R, Bautz WA, Janka R. Automated breast ultrasound: lesion detection and BI-RADS classification—a pilot study. Rofo. 2008;180(9):804-8.
Wojcinski S, Farrokh A, Hille U, Wiskirchen J, Gyapong S, Soliman AA, Degenhardt F, Hillemanns P. The Automated Breast Volume Scanner (ABVS): initial experiences in lesion detection compared with conventional handheld B-mode ultrasound: a pilot study of 50 cases. Int J Womens Health. 2011;3:337-46.
Zhang J, Lai XJ, Zhu QL, Wang HY, Jiang YX, Liu H, Dai Q, You SS, Xiao MS, Sun Q. Interobserver agreement for sonograms of breast lesions obtained by an automated breast volume scanner. Eur J Radiol. 2011; doi:10.1016/j.ejrad.2011.06.043
Preparing for a new future of naturopathic medicine in Ontario

Preparing for a new future of naturopathic medicine in Ontario
The process of Transition
Getting the New Rules Right
The Naturopathy Act and a new College for the naturopathic profession in Ontario is about much more than a change in who regulates naturopathic medicine in Ontario. The vision of the profession extending back to the 1980’s, and a major focus for OAND efforts and resources, has been to have a new foundation in legislation that helps to create new opportunities for collaboration, and contributes to the growing respect and understanding of the value of naturopathic medicine.
That is why the naturopathic profession is concerned that the government-appointed Transitional Council is having a challenge in developing the new rules for the profession under the Naturopathy Act. The goal is for these new rules to be approved and the new regulatory College in place by March, 2013.
When Transitional Council consulted on the draft regulations last fall, there was a clear consensus in the profession that the proposed new rules did not properly capture the scope of practice of the profession, and would create barriers to collaboration and integration of NDs that would both impact patient care, and limit the potential contribution of NDs to the healthcare system.
This profession’s view builds on the new scope of the profession in British Columbia. Jason Boxtart ND, the Chair of the Canadian Association of Naturopathic Doctors, said “The CAND supports legislation and regulations that ensure naturopathic doctors can practice to the full extent of their education and training. The professional associations, regulators and educational institutions in Canada, through the Canadian Naturopathic Coordinating Council (Chaired by the CAND) recognize the Scope of Practice and regulations in place in British Columbia as a “national scope of practice” for use in all jurisdictions. The CAND supports the OAND and all other provincial associations in their efforts to obtain effective and appropriate regulations for NDs in line with the BC model.”
Despite a widespread consensus in the profession that the proposed approach would needlessly leave Ontario as one of the most restrictive places to practice naturopathic medicine, Transitional Council chose to make no substantive changes. Council did issue a series of “Fact Sheets” intended to provide a rationale for their recommendations, but these lacked reference to any evidence about safety or training concerns, impacts on patient care, what is permitted in other jurisdictions, or broader health policy considerations.
The OAND and the profession remain engaged in efforts to work with the Ontario government to help identify needed changes to the draft regulations. At the same time, the OAND remains determined to build a stronger working relationship with Transitional Council, in keeping with best practices for a self-regulating health profession.
Getting transition right creates the potential for NDs to more fully emerge as a primary care profession. Particularly for patients interested in a more natural approach to health, it is important that NDs be able to use all their skills and training like they can in other jurisdictions, and be able to fully take their place as a collaborative and integrated profession.
Why a new foundation?
Ontario’s 1200 Naturopathic Doctors have been regulated since the 1920s under the Drugless Practitioners Act. Being the only health profession outside of the Regulated Health Professions Act has created many barriers to collaboration with other health professions and integration into the health care system. Antiquated legislation also makes it difficult for Ontario NDs to use all their skills and training, and to be able to introduce new therapies that are being safely and effectively used by NDs in places with more modern rules.
The 2007 Naturopathy Act moves the profession into the same regulatory framework as all other professions, and for the first time provides the profession with a clear scope and six controlled acts: diagnosis, prescribing, administering a substance, examinations and treatment beyond the openings of the body, blood draws, and manipulation. The Act also provides patients with proper confidence that there are the same mechanisms as other professions to allow complaints and discipline to be addressed fairly and effectively.
Ultimately, this new foundation recognizes the choice of naturopathic medicine as part of the mainstream of healthcare and provides the basis for more understanding and respect for the profession and practitioners, and helps NDs to more fully emerge as a primary care profession in the eyes of the public.
NDs and the Health Care System
This new foundation for the profession comes at a time when Ontario’s health care system is facing major challenges.
The growing cost of the health care system is clearly threatening its sustainability. Today, 43% of Ontario revenue is going to health care (Conference Board of Canada 2011). Unless new approaches are taken, health care costs will consume 80% of Ontario spending by 2030, taking resources away from all other provincial priorities (TD Economics 2010).
Little can be done about cost pressures resulting from population growth, inflation, and an aging population. But other cost drivers can be limited through new approaches. Most chronic diseases, from diabetes to cancer, are the product of modifiable health risks. The enrichment factor, including drug costs, new technologies and changing patients’ expectations can also be shifted (Ontario Ministry of Finance 2010). Changes in these areas are critical to sustaining the health care system.
New Approaches are Needed
Disease prevention is widely recognized as key to savings in the health care system (Toronto Star 2011). 80% of Ontarians over the age of 45 have a chronic disease (Ontario Ministry of Health and Long Term Care 2007). Over a million Ontarians have been diagnosed with diabetes, and this number is expected to increase by more than 60% over the next decade (Canadian Diabetes Association 2010). 80% of Canadians aged 20 to 59 have at least one of five major modifiable health risks, including hypertension, elevated cholesterol, and obesity (Makrides 2010). Pharmaceutical costs are rising fast, and recently overtook physicians as the second largest area of health spending in Ontario (TD Economics 2010). Nearly one third of drug costs are for conditions that are the result of modifiable health risks, including high cholesterol, high blood pressure, diabetes and stomach ulcers (Globe and Mail 2010). In fact drug costs are a particular impact for Ontario, where benefits are some of the most generous in the country (TD Economics 2010).
There is increasing recognition that NDs offer solutions to many of the biggest challenges in health care. The profession has been building awareness that NDs are clinically trained to play a larger role in the delivery of primary care, and to ensure that NDs are recognized for their unique expertise in wellness and addressing preventable risk factors, including chronic diseases.
The care provided by NDs contributes to managing major cost drivers in the public system through several avenues; NDs are experts in addressing prevention and modifiable risk factors, provide patients with alternatives to pharmaceuticals, provide a more personalized approach to medicine that is increasingly in demand, and provide access to primary care in particular for those wanting an alternative to conventional medicine.
With the clear challenges to the sustainability of the health care system, it is important that NDs be able to use all of their skills and training to provide patients with the care they want. Patients of ND’s are inherently proactive with their health thereby creating savings for the public healthcare system.
Other professions are also making changes to respond to increasing patient expectations that their health care choices will be respected. The new CPSO policy on Complementary/Alternative Medicine recognizes and supports patient-centred care, including respect for preferences, to incorporate non-allopathic approaches from their MD and other practitioners. Recognizing the legitimacy of non-allopathic therapies for primary or secondary care helps to foster a culture of respect for patient choice and for health care professionals practicing complementary medicine, and provides another foundation for improved collaboration.
References
Canadian Diabetes Association, Cost of Diabetes in Ontario, 2010
Conference Board of Canada, 2011 Budget: Controlling Growth in Health-Care Spending is Key to Budget Commitment to Balance the Books, website.
Globe and Mail, Insurers Focus on Prevention, January 3, 2010
Makrides L, Sawatzky C, Petrie J, Veinot P. Modifiable health risks in Atlantic Canadian employees: a 5-year report. Health Promot Int. 2010 Dec;25(4):384-93.
Ontario Ministry of Finance, Ontario’s Long Term Report on the Economy, 2010, Chapter 3.
Ontario Ministry of Health and Long Term Care, Preventing and Managing Chronic Disease – A Framework, 2007, p.3
TD Economics: Charting a Path to a Sustainable Health Care System, 2010, Pages 4-11.
Toronto Star, Illness Prevention Will Save Taxpayers Money: McGuinty, May 9, 2011.
WHO is deeply concerned by mutated birdflu research
The World Health Organization (WHO) issued a stern warning at the end of December 2011 to scientists who have engineered a highly pathogenic form of the deadly H5N1 bird flu virus, saying that their work carries significant risks and must be tightly controlled. WHO reported that it is “deeply concerned about the potential negative consequences” of work by two leading flu research teams who had said earlier in the month that they found ways to make H5N1 into an easily transmissable form capable of causing lethal human pandemics. In its first comment on the controversy, the WHO said: “While it is clear that conducting research to gain such knowledge must continue, it is also clear that certain research, and especially that which can generate more dangerous forms of the virus…has risks.” H5N1 bird flu is extremely deadly in people who are directly exposed to it from infected birds but so far it has not yet naturally mutated into a form that can pass easily from person to person. Scientists fear that this kind of mutation is likely to happen at some point and will constitute a major health threat if it does.
(Ambien)
Panel: Some men can delay prostate cancer treatment
An independent panel of experts convened by the U.S. National Institutes of Health (NIH) has reported that men with low-risk prostate cancer may want to wait to see if their disease progresses before receiving treatment. The panel backed the so-called active monitoring approach to prostate cancer treatment as a way to help men avoid the potential health consequences of treatment, which can include impotence and incontinence. Several studies have suggested that men are over-screened and over-treated for prostate cancer. “It’s clear that many men would benefit from delaying treatment,” said Dr. Patricia Ganz, a cancer prevention expert at the University of California Los Angeles, who chaired the NIH’s state-of-the-science panel on prostate cancer. The problem, said Ganz, is that there is no consensus on the best strategies for monitoring the progress of prostate cancer or on the benchmarks that should be used to determine when treatment is needed. “We need to standardize definitions, group patients by their risks and conduct additional research to determine the best protocols for managing low-risk disease,” she said in a statement. The panel urged NIH for more research to clarify this matter.
Advance® Xtra Performance (XP) male sling system launched in Canada
American Medical Systems (AMS), a leading provider of world-class devices and therapies for male and female pelvic health has announced the Canadian launch of AdVance XP, a minimally invasive implant for the treatment of male stress urinary incontinence (SUI). Male SUI is a common side effect of prostate cancer and benign prostatic hyperplasia treatments, such as radical prostatectomy and transurethral resection of the prostate. Built on the success of the AdVance platform, AdVance XP incorporates additional features that are designed to deliver Xtra Performance for improved ease-of-use and clinical outcomes. Enhancements include a redesigned sling that incorporates a new mesh designed to improve procedural reproducibility, longer arms that are easier to use in larger patients, and distinct tissue anchors designed to increase holding power during the critical healing period, following implantation. This latest Health Canada licensing and launch brings AdVance XP to North America for the first time and increases the total number of countries to twelve where this latest AMS innovation is being supplied to physicians and their patients.





