






Two postprandial crossover studies with healthy normal-weight male subjects were conducted to study the influence of commercial lingonberry (Vaccinium vitis-idaea L.) powder on postprandial glycemia and lipemia. The test meals contained fat-free yogurt with either glucose (50 g) or triacylglycerols (35 g) with or without the lingonberry powder. The lingonberry powder, which is a rich source of polyphenols, provided the meals with a known amount of fiber and a known amount and composition of sugars. Postprandial glucose, insulin, and triacylglycerol responses were analyzed. There were no significant differences in the postprandial glucose concentration between the meals in the glycemia trial despite the fact that the lingonberry meal contained more glucose and fructose. No glycemia or lipemia-lowering effects were detected when the meal contained added triacylglycerol without the added sugar. On the contrary, there were indications of higher glycemic and insulinemic effects after the lingonberry meal. The authors concluded that the fibers and/or polyphenols present in lingonberries null the glycemic effect of the sugars present in the berries when consumed together with added glucose. By contrast, the lingonberry powder did not affect the postprandial lipemic response. Nutr Res. 2012 Jul;32(7):471- 8. PMID: 22901554
Infant origins of childhood asthma associated with specific molds

This birth cohort study was conducted to examine whether specific mold exposures during infancy are associated with childhood asthma development. Infants were identified from birth certificates and when they reached eight months of age, dust samples were collected from 289 homes. The dust samples were analyzed for concentrations of 36 molds that comprise the Environmental Relative Moldiness Index (ERMI) and included the endotoxin, house dust mite, cat, dog, and cockroach allergens. Asthma was diagnosed in 24% of the children at age seven years based on reported symptoms and objective measures of lung function. A statistically significant increase in asthma risk was associated with high ERMI values in the child’s home in infancy (the adjusted relative risk for a 10-unit increase in ERMI value was 1.8; 95% CI 1.5-2.2). The summation of levels of the three mold species, Aspergillus ochraceus, Aspergillus unguis, and Penicillium variabile, was significantly associated with asthma (the adjusted relative risk was 2.2; 95% CI 1.8-2.7). The authors concluded that exposure to three mold species common to water-damaged buildings during infancy was associated with childhood asthma at age seven years. J Allergy Clin Immunol. 2012 Jul 10. PMID: 22789397
Low maternal folate status is associated with childhood emotional problems

This population-based cohort study (N = 3,209) assessed the association of maternal folate status during pregnancy with child emotional and behavioral problems at age three years. It also examined whether any association between folate status and child problems is a consequence of maternal folic acid supplement use or a variation in maternal MTHFR genotype (mothers of European descent were genotyped for the MTHFR 677 C→T polymorphism). Children of mothers with prenatal folate deficiency were at higher risk of emotional problems (OR 1.57; 95% CI 1.03-2.38) but not behavioral problems (OR 1.00; 95% CI 0.64-1.56) after adjustment for confounders. A higher risk of emotional problems was also found in children whose mothers started using folic acid supplements late or did not use supplements at all (OR 1.45; 95% CI 1.14-1.84) compared to children whose mothers started periconceptionally. However, low plasma folate concentrations only partly explained this association (OR 1.38; 95% CI 1.08-1.78). Although related to plasma folate concentrations, maternal MTHFR genotype did not explain the association of folate status with offspring emotional problems. Therefore, low maternal folate status during early pregnancy is associated with a higher risk of childhood emotional problems. Am J Clin Nutr. 2012 May 9. PMID: 22572645
Ubiquinol improves semen parameters in men with idiopathic infertility

This 26-week randomized, placebo-controlled trial investigated the effects of 200 mg ubiquinol (a reduced form of coenzyme Q10) daily on semen parameters in infertile men with idiopathic oligoasthenoteratozoospermia (N=228). After completion of the 26- week treatment phase, participants were followed for another 12-week off-drug period. Upon completion of the treatment period, sperm density in the ubiquinol and placebo groups was 28.7 × 10(6)/ml and 16.8 × 10(6)/ml (P = 0.005), sperm motility was 35.8% and 25.4% (P = 0.008), and sperm strict morphology was 17.6% and 14.8% (P = 0.01) of normal sperm, respectively. Serum follicle-stimulating hormone levels decreased (P = 0.02) and serum inhibin B concentrations increased (P = 0.01) during the treatment period. Although semen parameters gradually returned to baseline values during the offdrug period, differences remained significant for sperm density (P = 0.03) and sperm motility (P = 0.03). A positive association was found between the duration of treatment with ubiquinol and sperm density (r = 0.74, P = 0.017), sperm motility (r = 0.66, P = 0.024), and sperm morphology (r = 0.57, P = 0.027). Therefore, ubiquinol was effective for improving sperm parameters in men with unexplained oligoasthenoteratozoospermia. J Urol. 2012 Aug;188(2):526-31. PMID: 22704112
Soy isoflavone supplementation reduces body weight and improves glucose metabolism: meta-analysis

This meta-analysis was conducted to confirm the effects of soy isoflavone supplementation on body weight, fasting glucose, and insulin level in non-Asian postmenopausal women. PubMed, EMBASE, and Cochrane databases up to October 2010 were searched for randomized controlled trials; 9 studies with 528 participants for body weight, 11 studies with 1182 participants for fasting glucose, and 11 studies with 1142 participants for fasting insulin were included. Significant reductions were found in body weight (95% CI -0.895 to -0.134), glucose level (95% CI -0.344 to -0.033), and fasting insulin level (95% CI -1.721 to -0.159) with soy isoflavone supplementation compared to placebo. Furthermore, shorter duration of isoflavone supplementation (<6 mo) reduced body weight (P = 0.009) and longer duration of supplementation (≥6 mo) reduced blood glucose (P = 0.001). Greater weight loss reduction was observed in the lower dose subgroup (< 100 mg). Moreover, supplementation was more effective to reduce body weight and fasting insulin level in normal weight (BMI < 30) than obese (BMI ≥ 30) women. Therefore, soy isoflavone supplementation could be beneficial for body weight reduction, glucose, and insulin control in post-menopausal women. Nutrition. 2012 Aug 1. PMID: 22858192
Red wine influences gut microbiota ecology and biochemical biomarkers

This randomized, crossover, controlled intervention study was conducted to evaluate the effect of a moderate intake of red wine polyphenols on select gut microbial groups implicated in host health benefits. After a washout period, 10 healthy male subjects received red wine, the equivalent amount of de-alcoholized red wine, or gin for 20 days each. Total fecal DNA was submitted to polymerase chain reaction (PCR)-denaturing gradient gel electrophoresis and realtime quantitative PCR to monitor and quantify changes in fecal microbiota. Several biochemical markers were also measured. Compared with baseline, the daily consumption of red wine polyphenols significantly increased the number of Enterococcus, Prevotella, Bacteroides, Bifidobacterium, Bacteroides uniformis, Eggerthella lenta, and Blautia coccoides-Eubacterium rectale groups (P < 0.05). In parallel, systolic and diastolic blood pressures and triglyceride, total cholesterol, HDL cholesterol, and C-reactive protein concentrations decreased significantly (P < 0.05). Interestingly, changes in cholesterol and C-reactive protein concentrations were linked to changes in the bifidobacteria number. The authors concluded that red wine consumption can significantly modulate the growth of select gut microbiota in humans, suggesting a possible prebiotic benefit associated with the inclusion of red wine polyphenols in the diet. Am J Clin Nutr. 2012 May 2. PMID: 22552027
Ginger decreases pain in primary dysmenorrhea

This randomized, controlled trial was conducted to evaluate the effects of ginger on pain relief in moderate or severe primary dysmenorrhea (N = 120). The ginger and placebo groups in two different treatment protocols received 1500 mg of ginger root powder daily or placebo. In the first protocol, ginger and placebo were given two days before the onset of the menstrual period and continued through the first three days of the menstrual period. In the second protocol, ginger and placebo were given for the first three days of the menstrual period. Severity of pain was determined by a verbal multidimensional scoring system and a visual analogue scale. No differences were reported for baseline characteristics between the two groups. Significant differences were reported in the severity of pain between the ginger and placebo groups for protocol one (P = 0.015) and protocol two (P = 0.029). Protocol one (but not protocol two) also resulted in a significant difference in duration of pain (P = 0.017). Therefore, five days of treatment with ginger relieves the intensity and duration of pain in primary dysmenorrhea. BMC Complement Altern Med. 2012 Jul 10;12(1):92. PMID: 22781186
Salvestrols

Salvestrols
A natural, targeted approach to preventing and treating cancer
The ultimate goal in cancer research is to find a way to kill cancer cells present as tumors, precancerous lesions, or circulating cancer cells, and to accomplish this with minimal systemic toxicity. Any realistic evaluation of the current status to cancer therapy suggests that this goal is far from being achieved, although for a small number of cancers, achieving a complete and durable cure is possible.
This article describes an alternative approach to cancer prevention and therapy based on the remarkable properties of an enzyme highly expressed at the protein level in cancer cells and present only in negligible amounts in normal cells. This statement applies to at least 26 different cancer types. The reason this is important is that naturally occurring substrates for this enzyme exist which when metabolized in the cancer cell yield a cytotoxin that kills the cell. Research over the past decade has identified extracts of certain fruits that have been demonstrated in cell culture studies to provide highly active cytotoxic metabolites generated by this enzyme. In addition, serum variations in substrate and metabolite have been demonstrated to provide evidence of the presence of cancer, to some extent its stage, and when the substrate is observed to be metabolized and the metabolite detected, an indication of the success of the therapeutic intervention is evident. This provides compelling biological plausibility for the therapy and the action of this enzyme.
Human studies at this point in time involve case histories of 15 patients cured, in the opinion of the specialists involved, by the use of this oral therapy. The success of the therapy appears independent of the site. Given that this is a natural product, it is unrealistic at this time to expect more comprehensive clinical evidence, and to ignore this approach appears to be a serious mistake.
Introduction
The natural history of cancer indicates initiation via a modified cell is followed over a number of years by abnormal cell growth before there is any clinical evidence of the disease. Current technology involving either scanning or the use of biomarkers or reliance on clinical manifestation (e.g. a lump) has a threshold for detection of somewhere between 1/10th of a billion and one billion cells. The time from initiation to this tumor size ranges from a few years to as many as 20 years. An important feature of this process is that it is well advanced before diagnosis is currently possible (Burke 2009, O’Shaughnessy 2002). Multiple cancers may be present at a variety of stages of development, and patients may also already have established metastasis from the primary cancer prior to diagnosis or treatment. Millions of individuals currently have undetected, silent cancer that is somewhere between the initiation of a cancer cell and manifestation of the disease (Hyman 2007).
The challenge of primary prevention involves preventing the formation of the initial modified cells or detecting and destroying their progeny. Primary carcinogenesis appears to occur constantly due to mutations induced by natural background radiation or by cell changes induced by a variety of endogenous and exogenous factors. The fact that the human race is here today suggests the existence of one or more protective mechanisms. Put another way, why don’t we all get cancer? For existing tumours, the challenge is targeting with a localized therapy with low or negligible systemic toxicity, an approach attracting intense research interest at present (NIH 2012).
It is well established that the consumption of fruits and vegetables offers protection from cancer, and various constituents such as polyphenols have been suggested as responsible, partially mediated through the ability to counteract, reduce and also repair damage resulting from inflammation and oxidative stress (Reiss 2012, Seeram 2008, Vainio 2006, Ware 2009a). However, there is another mechanism which may be much more important. This is based on the fact that cancer cells express at the protein level an enzyme that is capable of metabolizing chemicals found in fruits and generating cytotoxic metabolites within the same cell. The enzyme belongs to the large P450 class and is designated CYP1B1. Already in 2002 it was reported that this enzyme converted resveratrol into the anticancer agent piceatannol (Potter 2002). So far, there are 26 cancer types where tumour cell overexpression of CYP1B1 has been demonstrated, but its presence in normal cells is negligible. In Appendix 1 of his book Linking Diet and Cancer. Salvestrols, Nature’s Defence Against Cancer, Dr. Brain Schaefer cites 62 studies (Schaefer 2012b). Taking advantage of this cytotoxin generating ability provides a targeted therapy independent of cancer type (Tan 2007).
The literature associated with exploiting the beneficial aspects of CYP1B1 is sparse and some appears in journals not covered by MEDLINE (PubMed). However, the book cited above provides a detailed, documented review of the issues being discussed here and also includes considerable unpublished information (Schaefer 2012b).
The search for the best CYP1B1 substrates
The remarkable property of CYP1B1 prompted two researchers, Professors Gerald Potter and Danny Burk in Leicester, U.K. to search for both synthetic and natural substrates using cancer cell culture techniques (Androutsopoulos 2008, Potter 2002, Potter 2006). A prodrug was developed and substrates for CYP1B1 yielding potent natural cytotoxic metabolites identified. In comparison with organically grown produce, produce grown with insecticides and from highly inbred varieties or hybridized to decrease bitterness had remarkably low levels of these substrates, an observation of great significance. The name Salvestrol was given to these active compounds or extracts (Schaefer 2012b, Tan 2007). They are vastly more selective than conventional chemotherapy because they target CYP1B1.
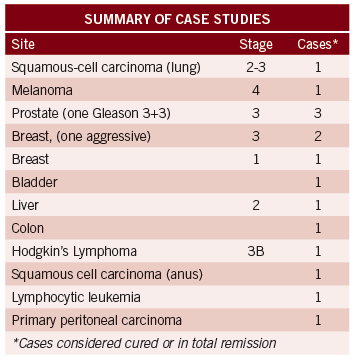
Summary of case studies
The evidence for human efficacy derives from a number of case studies. (Schaefer 2012a, Schaefer 2012b, Schaefer 2007, Schaefer 2010, Schaefer 2012c). In all cases listed in the table below, the cancer was considered cured by the oncologists involved. Additional cases have been collected including lung and pancreatic cancer (Schaefer 2012a).
Salvestrols of various potency were used by the individuals in these case studies which spanned a considerable time. Complete success is not always achieved by individuals using salvestrols, and dose, potency and adherence may be among the responsible factors. European experience with dose escalation suggests that there is a range of a factor of about two in the dose that produces response (Schaefer 2012a). Also, the currently available commercial extract is much more potent than earlier formulations. Dismissing or ignoring these case studies because they are not proper clinical trials is unrealistic considering a natural product is involved.
The author of this article attempted to give wider recognition to the remarkable property and potential of CYB1B1 and some of these results by publishing two articles, but there appears to be little interest (Ware 2009a, Ware 2009b). Instead, research interest is focused on inhibiting this enzyme because it is implicated in carcinogenesis, especially involving aromatic hydrocarbons and estrogen, or on research involving stimulating immune activity against CYP1B1 (McFadyen 2005, Swanson 2010). However, once one has cancer, this seems irrelevant. Inhibition of CYP1B1 would address only a very minor aspect of carcinogenesis while eliminating what appears to be a very important human defence mechanism against this disease. Also, smoking is an avoidable risk and the major source of exogenous aromatic hydrocarbons. Given the apparently universal phenomenon of CYTP1B1 overexpression in cancer cells, it is hard to see how this enzyme could have evolved to be anything other than mostly beneficial, and thus not a target for inhibition or a vaccine (which exists, incidentally).
Diagnosis by detecting CYP1B1 in serum
The original observation that CYP1B1 was not expressed in normal cells was found to be not universally true when highly sensitive detection methods were used, although the levels were still vastly lower than found in tumour tissue (Schaefer 2012b) Eventually the researchers developed a highly sensitive serum assay specific for human CYP1B1 protein. A proteomic approach was involved and it was possible to establish a baseline CYP1B1 level in individuals believed to be free of cancer which was minute but not zero. This background of CYP1B1 may reflect adventitious cancer cells constantly being generated. Based on thresholds derived from this background level, Schaefer estimates that the present level of sensitivity allows cancer detection about six years prior to clinical manifestation. For example, CYP1B1 at between 100 and 6000 times normal background was measured in lung cancer patients with levels providing a good correlation with the extent of disease (Schaefer 2012b).
Monitoring the success of therapy with serum CYP1B1 metabolites
Schaefer describes a second blood test termed the metabolic approach (Schaefer 2012b). A sensitive analytical method for testing in blood and urine for both the salvestrol (substrate) and its CYP1B1 metabolite was developed, and provided the opportunity to detect the presence of the enzyme and measure the extent of the cancer by the change in substrate concentration and the appearance of metabolite. A salvestrol was used that produced large amounts of metabolite with no confounding from dietary sources, and upon testing a group of healthy individuals it was found the salvestrol was recovered unmetabolized in the blood and urine. When cancer patients were given the salvestrol, the metabolite was found and the amount of substrate decreased with the magnitude of the effect dependent on the severity of the disease as estimated from the clinical presentation. For severe disease, the researchers were unable to detect any substrate, only the metabolite. These observations were made on individuals with breast, stomach, kidney, and prostate cancer with an array of stages but skewed towards more advanced cases. This approach does not yield site-specific information if the presence of cancer is indicated.
The metabolic approach obviously offers the opportunity to measure the effectiveness of any given salvestrol mixture, as well as the ability to examine and adjust for individual dose dependence. Finally a noninvasive judgment is possible regarding when a “cure” or significant regression has been achieved by this alternative approach. This can then be confirmed by conventional methods.
The proteomic approach is exquisitely sensitive and close to the state of the art for detection of a chemical in the circulation. Thus if screening is done and a positive result is obtained, where is the cancer? A serious problem since it may be small enough as to escape all modern attempts to locate it. Also, there is no non-specific anticancer treatment in so-called evidence based or officially sanctioned cancer therapy that could be used in the absence of knowledge of the identity of the tumour site. But the metabolic approach allows testing the most modern and powerful salvestrol on patients with cancer, even if not clinically evident, to determine if the metabolic markers change, thus potentially justifying and encouraging an alternative therapeutic program, independent of the lack of knowledge of the actual site.
The future
Mainstream medicine thinks only in terms of their holy grail, the randomized, controlled trial as evidence for even considering a new therapy. Held in high contempt is the case study. Consider the obstacles facing salvestrols. Naturally occurring chemicals generally cannot be patented. Companies selling products such as salvestrols are tightly regulated as to what claims can be made concerning efficacy. Clinical trials required for regulatory approval are very expensive. Only a synthetic salvestrol has a chance of becoming an approved prescription drug or approved “medicinal food.” It would be hard to find a physician who would take the professional risk of recommending to a cancer patient a natural product rather than the conventional approach. Combining salvestrols with conventional treatment is interesting but probably would be hard to implement in the face of negative attitudes.
A trial can be visualized that might satisfy integrative physicians demanding more concrete evidence. It would involve patients who have rejected conventional treatment or found it failed them. These individuals could be recruited for an uncontrolled study or an old-fashioned study where the control is based on the average life expectancy or cancer progression of multiple matched untreated patients.
Taking low doses of salvestrols for cancer prevention also appears reasonable and this may be significantly superior to taking fruit extracts available at the health food store or online because salvestrols are selected extracts which have laboratory-proven cancer cell cytotoxicity. The above discussion provides justification for the role of salvestrols in prevention. However, the optimum dose is still unknown.
Conclusions
The underlying theory of salvestrols is that CYP1B1 represent a rescue enzyme that evolved in humans eons ago, partly in order to deal with cancer cells and destroy them with substances derived from the normal diet. The evidence is compelling that this enzyme is overexpressed in cancer cells and present only in minute and insignificant levels in normal cells. Furthermore, related to diagnosis and prognosis, the enzyme is present at vastly higher levels in the blood of individuals with cancer as compared to those who are cancer free. The observations based on cell culture studies involving cancer and normal cells confirm the presence of cytotoxic metabolites of CYP1B1 and the indifference of normal cells to the substrate. When cancer patients are compared to normal controls, after dosing with salvestrols the serum salvestrol levels, rather than being unchanged, are lower and can be driven to near zero in advanced cancer patients, while evidence of toxic metabolites increases in step with these decreases. These observations significantly support the biological plausibility of the therapy. The modern salvestrols used in today’s preparations contain fruit-derived CYP1B1 substrates proven in cell culture studies to yield high levels of cancer cell cytotoxicity, whereas commercially available fruit extracts and polyphenols mixtures sold as supplements have never been graded for efficacy by this standard.
Evidence of salvestrol induced remission or cure consists of 15 specialist verified human case studies covering 11 cancer types. More are about to be reported. At this stage in the evolution of salvestrol therapy, this is the only clinical evidence one should expect. These case studies along with serum metabolite and proteomic studies support the salvestrol concept. While it is understandable that practitioners would be less than happy about such a modest clinical evidence base, it must be remembered that this is a natural product. There are even restrictions on the extent to which it can be promoted as effective against cancer and represents a therapy resisted a priori by conventional medicine. There will no doubt be small clinical trials in the near future, but given the absence of side effects of, waiting for such trials seems unnecessary. There are fewer regulatory barriers to the acceptance of the metabolic and proteomic approaches to cancer detection and monitoring therapy. This in fact is a principal focus at present with research ongoing at University of Victoria and University of British Columbia (Schaefer 2012a).
Issues such as the use of salvestrols for primary and metastatic cancer prevention will no doubt remain theoretical for a long time, given the natural history of cancer and nature of the product, and the huge cost of human studies. Nevertheless, to ignore the possibility that this is a true magic bullet with minimal or no side effects may be to ignore one of the most important developments in cancer detection and therapy in decades.
Salvestrols are availble at www.salvestrol.ca. Dr. Schaefer’s book can be ordered via this link: http:// www.salvestrolbook.com.
Disclaimer and conflict of interests
The author of this article has no financial interest in any commercial or research aspect of salvestrols, does take daily low dose of Salvestrol “Platinum” for prevention, and emphasizes that the above review does not constitute a recommendation or advice but merely provides information.
References
Androutsopoulos,V., Arroo,R.R., Hall,J.F., Surichan,S. and Potter,G.A. Antiproliferative and cy-tostatic effects of the natural product eupatorin on MDA-MB-468 human breast cancer cells due to CYP1-mediated metabolism. Breast Cancer Res 2008; 10(3): R39.
Burke,D. The silent growth of cancer and its implications for nutritional protection. British Neu-ropathic Journal 2009; 26(1): 15-18.
Hyman,M.A. Cancer–treatment through the continuum. Altern. Ther Health Med 2007; 13(1): 10.
McFadyen,M.C. and Murray,G.I. Cytochrome P450 1B1: a novel anticancer therapeutic target. Future Oncol 2005; 1(2): 259-263.
NIH, 2012. Targeted Cancer therapies. Fact sheet, National Institutes of Health. http://www.cancer.gov/cancertopics/factsheet/Therapy/ Fs7_49.pdf.
O’Shaughnessy,J.A., Kelloff,G.J., Gordon,G.B., Dannenberg,A.J., Hong,W.K., Fabian,C.J., Sig-man,C.C., Bertagnolli,M.M., Stratton,S.P., Lam,S., Nelson,W.G., Meyskens,F.L., Alberts,D.S., Follen,M., Rustgi,A.K., Papadimitrakopoulou,V., Scardino,P.T., Gazdar,A.F., Wattenberg,L.W., Sporn,M.B., Sakr,W.A., Lippman,S.M. and Von Hoff,D.D. Treatment and prevention of intraepi-thelial neoplasia: an important target for accelerated new agent development. Clin Cancer Res 2002; 8(2): 314-346 see Fig.1.
Potter,G.A. and Burke,M.D. Salvestrols–Natural products with tumour selective activity. Journal of Orthomolecular Medicine 2006; 21(1): 34-36.
Potter,G.A., Patterson,L.H., Wanogho,E., Perry,P.J., Butler,P.C., Ijaz,T., Ruparelia,K.C., Lamb,J.H., Farmer,P.B., Stanley,L.A. and Burke,M.D. The cancer preventative agent resveratrol is converted to the anticancer agent piceatannol by the cytochrome P450 enzyme CYP1B1. Br. J Cancer 2002; 86(5): 774-778.
Reiss,R., Johnston,J., Tucker,K., Desesso,J.M. and Keen,C.L. Estimation of cancer risks and benefits associated with a potential increased consumption of fruits and vegetables. Food Chem Toxicol 2012.
Schaefer,B., 2012a. Personal communication.
Schaefer,B., 2012b. Salvestrols. Nature’s Defence Against Cancer. Linking diet and cancer. Clini-cal Intelligence Corp.
Schaefer,B.A., Hoon.L.T., Burke,M.D. and Potter,G.A. Nutrition and Cancer: Salvestrol Case Studies. Journal of Orthomolecular Medicine 2007; 22(4): 177.
Schaefer,B., Dooner,C., Burke,D. and Potter,G. Nutrition and Cancer: Further case studies involv-ing savlestrol. Journal of Orthomolecular Medicine 2010; 25(1): 17-23.
Schaefer,B., Potter,G., Wood,R. and Burke D Cancer and related case studies involving salvestrol and CYP1B1. Journal of Orthomolecular Medicine 2012c; 27(3): 131-138.
Seeram,N.P. Berry fruits for cancer prevention: current status and future prospects. J Agric. Food Chem. 2008; 56(3): 630-635.
Swanson,H.I., Njar,V.C.O., Yu,Z., Castro,D.J., Gonzalez,F.J., Williams,D.E., Huang,Y., Kong,A.N., Doloff,J.C., Ma,J., Waxman,D.J. and Scott,E.E. Targeting drug-metabolizing en-zymes for effective chemoprevention and chemotherapy. Drug Metabolism and Disposition 2010; 38(4): 539-544.
Tan,H.L., Butler,P.C., Burke,M.D. and Potter,G.A. Salvestrols: A New Perspective in Nutritional Research. Journal of Orthomolecular Medicine 2007; 22(1): 39-47.
Vainio,H. and Weiderpass,E. Fruit and vegetables in cancer prevention. Nutr Cancer 2006; 54(1): 111-142.
Ware,W.R. Nutrition and the prevention and treatment of cancer: association of cytochrome P450 CYP1B1 with the role of fruit and fruit extracts. Integr Cancer Ther 2009a; 8(1): 22-28.
Ware,W.R. P450 CYP1B1 mediated fluorescent tumor markers: a potentially useful approach for photodynamic therapy, diagnosis and establishing surgical margins. Med Hypotheses 2009b; 72(1): 67-70. 060-064.IHP_Feature2-v2.indd 58 12
Hyperthermia in Oncology

Hyperthermia in Oncology
A Hot Topic
Hyperthermia (HT), or thermal therapy, is the use of high temperature or heat against cancerous tissues. This article will look at local-regional HT, which has historically been used in some form or another across most ancient medical traditions. Naturopathic training includes the use of various local therapeutic heat treatments including hydrotherapy, moxibustion, herbs such as cayenne, heating pads, diathermy, and others. More recently, HT has been studied alongside radiotherapy and chemotherapy, and has been shown to act as a chemotherapy and radiotherapy sensitizer. There has also been a significant amount of literature published on the immune effects of HT, including HT’s ability to modulate cells of the innate and adaptive immune systems. By multiple mechanisms, HT treatments have been shown to significantly improve local tumour control and provide a survival advantage in many solid cancers. Some human trials published in the literature have been contradictory, largely due to differing experimental temperatures and exposure times. This article reviews the evidence available and describes various potential mechanisms of action that HT exerts on the immune system. Clinical pearls from the practice of a Fellow of the American Board of Naturopathic Oncology are provided.
Introduction
HT is a procedure whereby the temperature of cancerous tissue is increased above what is considered normal, most often in the 40-43 degrees Celsius range (Wust 2002). Through multiple mechanisms, including direct cell killing, treatments have the ability to significantly improve local tumour control and provide a survival advantage to cancer patients (Dewey 1994). HT can also act as a chemotherapy and radiation sensitizer (Jones 2003). HT can modulate directly or indirectly the cells of the innate and adaptive immune systems (Frey 2012). HT can improve tumour oxygenation, in both diffusion-limited and perfusionlimited hypoxic cells, which reverses the incapacitating effects of hypoxia in the tumour microenvironment and improves treatment outcomes (Song 2001). Finally, HT can inactivate superoxide dismutase (SOD) and allow tumours can be destroyed by inducing oxidative stress (Lehmann 2012). There are multiple forms of HT, such as whole body HT, but this paper will focus on local-regional HT. Even though HT may appear to be a promising adjunctive therapy, there have been contradictory results published in the literature. One argument is that the inconsistent outcomes after HT are due to differing experimental temperatures and exposure times (Frey 2012). The challenges in utilizing HT include heating tumours to high temperatures in a precise and reproducible manner, defining and calculating the required thermal dose for efficacy, and appropriately measuring temperature. There has been significant progress on all these issues, particularly in the last decade. This article will review the evidence available and describe various potential mechanisms of action of HT on the immune system. Clinical pearls from the practice of a Fellow of the American Board of Naturopathic Oncology will be provided.
Immune Effects of Hyperthermia
HT has general and specific effects on the innate and adaptive immune responses, similar and beyond that of fever. Studies have shown that HT has beneficial effects on macrophages. In one trial, the experimenters measured the response of macrophages to phytohaemagglutinin, a lectin that is used to measure cell-mediated immunity (Manzella 1979). It was found that even mild HT increased macrophage responsiveness. Higher temperatures, even if not above 40 degrees Celsius, can influence lymphocyte transformation and mitogenesis, both of which increase the activity of the immune system (Skeen 1983). A study that examined whole body HT in mice showed that HT influences the migration of Langerhans cells (Ostberg 2000). Langerhans cells are the dendritic cells of the skin and mucosa. As such, they are responsible for taking up microbial antigens and other antigens and acting as antigen-presenting cells. The systemic activation of the immune system by HT may help target metastatic tumour cells (von Ardenne 1972).
Heat shock proteins (HSPs) are proteins than can be induced by physiological stress, including environmental stresses and pathological states such as fever and inflammation (Morimoto 1993). They have immunomodulatory functions and can have positive and negative effects on regulating macrophage function, depending on the cellular location of the HSPs. Extracellular or membrane-bound HSPs might serve as a danger signal to stimulate the immune response (Schmitt 2007). HSPs are synthesized in response to HT treatments. In one study looking at HSP72, it was found to be expressed on the surface of malignant cells but not on normal cells (Multhoff 1995). HSPexpressing cells are more susceptible to lysis by natural killer (NK) cells. HSPs are released after necrosis and in turn then stimulate macrophage and dendritic cells to secrete cytokines, which can inhibit tumour development and progression (Basu 2000). HSPs may also act to repair or limit damage to otherwise healthy cells, protect them from or prevent future damage, or place the cells in a state that limits expression or fixation of damage (Tomasovic 1989). The exact mechanism is unclear.
Macrophage function can also be enhanced through an increased secretion of tumour necrosis factor (TNF), formerly known as TNF-alpha. Mild acute or chronic HT can increase tumour cell susceptibility to TNF (Tomasovic 1989). In vitro, TNF has effects on tumour vasculature and TNF-mediated cell killing is stimulated by chronic heating (Ruff 1981). Studies that have examined the effects on macrophages of potential treatment sequences have shown that appropriately constructed sequences for macrophage priming and triggering combined with HT could augment the cytotoxic actions of macrophages, which could have important clinical implications (Tomasovic 1989).
NK cells have the ability to detach from tumour cells and kill novel tumour cells (Bhat 2007). However, there is some conflicting evidence on the way HT influences them. NK cell activity is modified by their environment and seems to be impaired in various cancer types, including lymphoma, breast cancer, and multiple myeloma (Konjevic 2012). HT at temperatures above 40 degrees Celsius has been shown to decrease NK cell activity in many in vitro studies (Azocar 1982). However, whole body HT has been shown to increase NK cell activity in vivo (Zanker 1982). Despite the conflicting evidence at higher temperature ranges, there is evidence that fever-range thermal stress at a temperature of 39.5 degrees enhances NK cell cytotoxicity against tumour cells (Dayanc 2008).
Hyperthermia Trials
Several older non-randomized trials have looked at the use of HT alone and in combination with other therapies. A review of 14 studies looking at HT by itself with 343 patients demonstrated complete response rates varying from 0-40%, with an overall complete response rate of 13% (Hetzel 1987). However, these studies found that using HT alone resulted in a short duration of response. The first two randomized studies failed to show a beneficial effect of adding HT to radiotherapy (van der Zee 2002). One criticism of these initial randomized trials was that the treatment techniques were inadequate for the patients included. Since then, many trials have examined the use of HT in conjunction with either chemotherapy, radiotherapy, or with both. The large majority have shown significantly better results with the HT group (van der Zee 2002).
A review looking at selected phase I, II, and III trials investigated the effects of HT combined with radiotherapy, chemotherapy, or both, obtained data on 2200 patients (Falk 2001). The trials it analyzed had been performed in patients with a variety of solid tumours including: melanoma, head and neck cancer, breast cancer, cancer of the gastrointestinal tract or urogenital tract, glioblastoma, and sarcoma. The authors concluded that although the effects of HT vary depending on cancer type, complete response rates with HT, alone or in combination with other therapies is possible (Falk 2001).
One of the most compelling studies involved randomizing patients with metastatic stage IV squamous cell cancer of the head and neck to radiotherapy, or to radiotherapy plus HT (Overgaard 1995). In this trial, the complete response rate improved from 41% to 83%, with 5-year overall survival increasing from 0% to 53% with the addition of HT (Valdagni 1993). Another compelling study analyzed the results of five randomized controlled trials in the treatment of superficial localized breast cancer (Vernon 1996). This study included over 300 patients who had advanced primary or recurrent breast cancer and in which local radiotherapy was indicated. Not all trials demonstrated an advantage for the combined treatment, but the overall complete response rate for radiotherapy alone was 41% and for the combined treatment was 59%. The greatest effect was in patients with recurrent lesions where further irradiation was limited to low doses (Vernon 1996). Local HT appears to follow a dose-response relation, in that the number of treatments is related to the degree of local tumour control (Wust 2002). There are doseresponse relationships between temperature and killing effects as well. These vary depending on cell lines and tumour types (Dewhirst 1980).
Another study examined the effect of adjuvant interstitial HT in patients with glioblastoma undergoing brachytherapy boost after conventional radiotherapy (Sneed 1998). In this study, adults with newly-diagnosed glioblastoma were randomized and treated with partial brain radiotherapy. Those patients whose tumour was still implantable after teletherapy were randomized to brachytherapy boost with or without HT for 30 minutes immediately before and afterwards. 79 patients were randomized between the two groups. Both endpoints that were measured (time to progression and survival) were significantly longer for HT than without HT, regardless of the use of brachytherapy (Sneed 1998).
HT can be utilized for many types of malignancy. In one study, patients with advanced adenocarcinoma and severely symptomatic benign prostatic hyperplasia received transrectal microwave HT of the prostate (Szmigielski 1991). Local HT was given twice a week for a total of six sessions and the treatments were administered using a water-cooled rectal applicator. Each session lasted for 30 minutes and the rectal mucosa temperature was controlled at 45 degrees Celsius. The results indicated a significant increase in NK cell cytotoxic activity in the adenocarcinoma patients, indicating a transient stimulation of cell-mediated immune reaction (Szmidielski 1991).
Finally, a more recent randomised phase 3 multicentre study investigated the use of regional HT with chemotherapy in high-risk soft-tissue sarcoma (Issels 2010). Prior to these, phase 2 studies showed that the combination of HT and chemotherapy improved local control compared to chemotherapy alone. In the phase 3 study, patients were randomly assigned to receive chemotherapy alone or combined with regional HT in addition to local therapy. 341 patients were enrolled in total, with approximately half in each group. Patients had higher progression rates and death rates with chemotherapy alone. The treatment response rate in the group that received HT was 28.8%, compared with 12.7% in the chemotherapy alone group. The adverse events associated with HT included pain, pressure, and skin burn (Issels 2010). Overall, HT appeared to improve patient outcomes and was a valuable addition to chemotherapy.
Clinical Pearls
Dr. Gurdev Parmar, ND, FABNO is the co-founder and medical director of the Integrated Health Clinic (IHC) in Fort Langley, British Columbia. Dr. Parmar has been using local-regional HT with patients since 2009 and fever-range whole body HT for the past year. At the IHC, local-regional HT has now been used with over 250 patients, totalling over 3500 treatments. This has given Dr. Parmar and his team an opportunity to use this treatment against many different tumour types and at varying stages of disease. The IHC is finalizing a database for all patients treated thus far with HT. Dr. Parmar will be presenting the basic data from this database soon at the 41st annual International Clinical Hyperthermia Society conference in Budapest. The rest of the more detailed retrospective data is slated to be published in early 2013.
Dr. Parmar is also working on a prospective study that is moving forward. He reports having noticed a significant benefit to many of his patient’s quality of life and overall survival when adding HT to their treatment plan. He looks forward to the day that HT is widely available to patients across the country and the world. It is Dr. Parmar’s contention that HT will be the fourth pillar of conventional oncology care, as it improves the efficacy of chemotherapy and radiotherapy without any risk of interference. It also can be used as a salvage therapy once conventional measures have been exhausted, while maintaining a good quality of life, as there are few potential side effects or risks.
Conclusion
HT is a treatment strategy whereby the temperature of cancerous tissues is increased above normal. This paper focused largely on local-regional HT. HT is best used in combination with chemotherapy and radiotherapy, and can also be utilized in the late treatment of various cancers as a standalone therapy, or as a salvage therapy. Among its various possible mechanisms of action, much research has been conducted on the stimulating effects of HT on the innate and adaptive immune systems. HT appears to stimulate the activity of macrophages, NK cells, and also has immunomodulatory functions via the creation of HSPs. Elevated temperatures influence lymphocyte transformation and mitogenesis, both of which increase the activity of the immune system. The systemic activation of the immune system by HT may help target metastatic tumour cells.
HT is an effective chemosensitizer and radiosensitizer. HT also increases the amount of oxygen in the target tissue, which makes chemotherapy and radiotherapy function more effectively. In studies where HT has been used as a standalone therapy, response rates have been varied but impressive. HT has been studied in numerous cancer types, including melanoma, head and neck cancer, breast cancer, cancer of the gastrointestinal tract or urogenital tract, glioblastoma, sarcoma, and others. It is encouraging that the large majority of the research across various cancer types demonstrates that HT is an effective oncological treatment that can improve response rates and patient survival. Clinical experience from the practice of a Fellow of the American Board of Naturopathic Oncology in the treatment of over 250 patients has mirrored these findings. Finally, the most recent and best-conducted trials have shown that HT provides benefits above and beyond conventional oncological treatment approaches with minimal side effects.
References
Azocar J, Yunis EJ, Essex M. Sensitivity of human natural killer cells to hyperthermia. Lancet. 1982;1(8262):16-7.
Basu S, Binder RJ, Suto R, Anderson KM, Srivastava PK. Necrotic but not apoptotic cell death releases heat shock proteins, which deliver a partial maturation signal to dendritic cells and activate the NF-kappa B pathway. Int Immunol. 2000;12(11):1539-46.
Bhat R, Watzl C. Serial killing of tumor cells by human natural killer cells–enhancement by therapeutic antibodies. PLoS One. 2007;2(3):e326.
Dayanc BE, Beachy SH, Ostberg JR, Repasky EA. Dissecting the role of hyperthermia in natural killer cell mediated anti-tumor responses. Int J Hyperthermia. 2008;24(1):41-56.
Dewey WC. Arrhenius relationships from the molecule and cell to the clinic. Int J Hyperthermia. 1994;10(4):457-83.
Dewhirst MW, Ozimek EJ, Gross J, Cetas TC. Will hyperthermia conquer the elusive hypoxic cell? Implications of heat effects on tumor and normal-tissue microcirculation. Radiology. 1980;137(3):811-7.
Falk MH, Issels RD. Hyperthermia in oncology. Int J Hyperthermia. 2001;17(1):1-18.
Frey B, Weiss EM, Rubner Y, Wunderlich R, Ott OJ, Sauer R, Fietkau R, Gaipl US. Old and new facts about hyperthermiainduced modulations of the immune system. Int J Hyperthermia. 2012;28(6):528-42.
Harris JW, Meneses JJ. Effects of hyperthermia on the production and activity of primary and secondary cytolytic T-lymphocytes in vitro. Cancer Res. 1978;38(4):1120-6.
Hetzel FW, Mattielo J. Interactions of hyperthermia with other modalities. In Paliwal BR, Hetzel FW, Dewhirst MW, eds. Medical Physics Monograph no. 16: Biological, physical and clinical aspects of hyperthermia. College Park, MD: American Institute of Physics. 1987;30-56.
Issels RD, Lindner LH, Verweij J, Wust P, Reichardt P, Schem BC, Abdel-Rahman S, Daugaard S, Salat C, Wendtner CM, Vujaskovic Z, Wessalowski R, Jauch KW, Durr HR, Ploner F, Baur-Melnyk A, Mansmann U, Hiddemann W, Blay JY, Hohenberger P, European Organisation for Research and Treatment of Cancer Soft Tissue and Bone Sarcoma Group (EORTC-STBSG), European Society for Hyperthermic Oncology (ESHO). Neo-adjuvant chemotherapy alone or with regional hyperthermia for localised high-risk soft-tissue sarcoma: a randomised phase 3 multicentre study. Lancel Oncol. 2010; 11(6):561-70.
Jones EL, Samulski TV, Dewhirst MW, Alvarez-Secord A, Berchuk A, Clarke-Pearson D, Havrilesky LJ, Soper J, Prosnitz LR. A pilot Phase II trial of concurrent radiotherapy, chemotherapy, and hyperthermia for locally advanced cervical carcinoma. Cancer. 2003;98(2):277-82.
Konjevic G, Jurisic V, Jovic V, Vuletic A, Mirjacic Martinovic K, Radenkovic S, Spuzic I. Investigation of NK cell function and their modulation in different malignancies. Immunol Res. 2012;52(1- 2):139-56.
Lehmann K, Rickenbacher A, Jang JH, Oberkofler CE, Vonlanthen R, von Boehmer L, Humar B, Graf R, Gertsch P, Clavien PA. New insight into hyperthermic intraperitoneal chemotherapy: induction of oxidative stress dramatically enhanced tumor killing in vitro and in vivo models. Ann Surg. 2012;256(5):730-8.
Manzella JP, Roberts NJ Jr. Human macrophage and lymphocyte responses to mitogen stimulation after exposure to influenza virus, ascorbic acid, and hyperthermia. J Immunol. 1979;123(5):1940-4.
Morimoto RI. Cells in stress: transcriptional activation of heat shock genes. Science. 1993;259(5100):1409-10.
Multhoff G, Botzler C, Wiesnet M, Muller E, Meier T, Wilmanns W, Issels RD. A stress-inducible 72-kDa heat-shock protein (HSP72) is expressed on the surface of human tumor cells, but not on normal cells. Int J Cancer. 1995;61(2):272-9.
Ostberg JR, Patel R, Repasky EA. Regulation of immune activity by mild ( fever-range) whole body hyperthermia: effects on epidermal Langerhans cells. Cell Stress Chaperones. 2000;5(5):458-61.
Overgaard J, Gonzalez Gonzalez D, Hulshof MC, Arcangeli G, Dahl O, Mella O, Bentzen SM. Randomised trial of hyperthermia as adjuvant to radiotherapy for recurrent or metastatic malignant melanoma. European Society for Hyperthermic Oncology. Lancet. 1995;345(8949):540-3.
Redmann K, Burmeister J, Jenssen HL. The influence of hyperthermia on the transmembrane potential, zeta-potential and metabolism of polymorphonuclear leukocytes. Acta Bio Med Ger. 1974;33(2):187-96.
Ruff MR, Gifford GE. Rabbit tumor necrosis factor: mechanism of action. Infect Immunol. 1981;31(1):380-5.
Schildkopf P, Ott OJ, Frey B, Wadepohl M, Sauer R, Fietkau R, Gaipl US. Biological rationales and clinical applications of temperature controlled hyperthermia–implications for multimodal cancer treatments. Curr Med Chem. 2010;17(27):3045-57.
Schildkopf P, Frey B, Ott OJ, Rubner Y, Multhoff G, Sauer R, Fietkau R, Gaipl US. Radiation combined with hyperthermia induces HSP70-dependent maturation of dendritic cells and release of proinflammatory cytokines by dendritic cells and macrophages. Radiother Oncol. 2011;101(1):109-15.
Schmitt E, Gehrmann M, Brunet M, Multhoff G, Garrido C. Intracellular and extracellular functions of heat shock proteins: repercussions in cancer therapy. J Leukoc Biol. 2007;81(1):15-27.
Skeen MJ, Olkowski ZL, DuPre JR, McLaren JR. Mitogenesis in human lymphocytes following brief exposure to hyperthermia. Int J Radiat Oncol Biol Phys. 1983;9(1):61-6.
Sneed PK, Stauffer PR, McDermott MW, Diederich CJ, Lamborn KR, Prados MD, Chang S, Weaver KA, Spry L, Malec MK, Lamb SA, Voss B, Davis RL, Wara WM, Larson DA, Phillips TL, Gutin PH. Survival benefit of hyperthermia in prospective randomized trial of brachytherapy boost +/- hyperthermia for glioblastoma multiforme. Int J Radiat Oncol Biol Phys. 1998;40(2):287-95.
Song CW, Park H, Griffin RJ. Improvement of tumor oxygenation by mild hyperthermia. Radiat Res. 2001;155(4):515-28.
Szmigielski S, Sobczynski J, Sokolska G, Stawarz B, Zielinski H, Petrovich Z. Effects of local prostatic hyperthermia on human NK and T cell function. Int J Hyperthermia. 1991;7(6):869-80.
Takada Y, Sato EF, Nakajima T, Hosono M, Tsumura M, Inoue M, Yamada R. Granulocyte-colony stimulating factor enhances anti-tumour effect of hyperthermia. Int J Hyperthermia. 2000;16(3):275-86.
Tomasovic SP, Klostergaard J. Hyperthermic modulation of macrophagetumor cell interactions. Cancer Metastasis REv. 1989;8(3):215-29.
Wust P, Hildebrandt B, Sreenivasa G, Rau B, Gellermann J, Riess H, Felix R, Schlag PM. Hyperthermia in combined treatment of cancer. Lancet Oncol. 2002;3(8):487-97.
Valdagni R, Amichetti M. Report of long-term follow-up in a randomized trial comparing radiation therapy and radiation therapy plus hyperthermia to metastatic lymph nodes in stage IV head and neck patients. Int J Radiat Oncol Biol Phys. 1994;28(1):163-9.
van der Zee J. Heating the patient: a promising approach? Ann Oncol. 2002;13(8):1173-84.
Vernon CC, Hand JW, Field SB, Machin D, Whaley JB, van der Zee J, van Putten WL, van Rhoon GC, van Dijk JD, Gonzalez Gonzalez D, Liu FF, Goodman P, Sherar M. Radiotherapy with or without hyperthermia in the treatment of superficial localized breast cancer: results from five randomized controlled trials. International Collaborative Hyperthermia Group. Int J Radiat Oncol Biol Phys. 1996;35(4):731-44.
von Ardenne M. Selective multiphase cancer therapy: conceptual aspects and experimental basis. Adv Pharmacol Chemother. 1972;10:339-80.
Zanker KS, Lange J. Whole body hyperthermia and natural killer cell activity. Lancet. 1982;1(8280):1079-80.
Female Fertility

Female Fertility
Oxidant stress and a potential role for antioxidant therapy
Infertility affects up to 15% of Canadian couples and may be attributed to a number of diverse factors. Recent evidence suggests that while oxidative processes play an essential role in human reproduction, a state of oxidative stress may contribute significantly to the inability to conceive.Oxidative stress has been implicated in endometriosis, recurrent pregnancy loss and poor embryo quality. Human studies into the effect of antioxidants upon reproductive outcomes have shown some promising results. Interventions including vitamin A, vitamin E, n-acetyl cysteine, and melatonin may quench oxidative stress, while observational data suggests a possible role for CoQ10. Antioxidants may offer novel therapeutic options in the management of female infertility.
Infertility is defined as a “failure to achieve a successful pregnancy after 12 months or more of regular unprotected intercourse” (PCASRM 2008). Recent surveys suggest that between 11.5% and 15.7% of Canadian couples attempting to get pregnant are dealing with an inability to conceive, with prevalence rates increasing with advancing maternal age (Bushnik 2012). It is estimated that approximately 30% of infertility causes may be attributed to male factors and 40% to female factors. In the remainder of cases, a combination of influences or an undetermined cause are deemed to be responsible (AHRC 2010).
Through diagnostic imaging and laboratory assessment, many causes of female infertility may be identified and treated. Common causes include disturbances to ovulation caused by polycystic ovarian syndrome (PCOS) and its accompanying insulin resistance and androgen dominance, and disruptions to the physical structure of the reproductive tract as a result of fibroids, endometriosis and pelvic inflammatory disease. Factors external to the reproductive tract such as age, genetics, smoking status and toxin exposure history can also influence the viability of reproductive cells and the success of attempts at pregnancy.
Endocrine functioning, involving the complex interplay of reproductive hormones (estrogen, progesterone, luteinizing hormone and follicle stimulating hormone), thyroid hormones (thyroid stimulating hormone, T3, T4, reverse T3), prolactin, melatonin, insulin and cortisol, has an equally important role in determining the success or failure of any attempts at conception. This component presents perhaps the greatest challenge to those working to support conception. Factors such as body composition, dietary choices, exercise and exposure to stress may have significant impacts on the functioning of this elegant, dynamic system.
In spite of our ability to image, measure and quantify so many aspects of the reproductive tract, a clear cause of infertility cannot be identified in a number of cases (Ledger 2009). These unexplained cases may be attributed in the future to other pathological processes that are the subject of current research including immune functioning (Siam 2011), genetic enzymatic variants (Eloualid 2012) and signaling peptides (Sadeu 2012). A role of oxidative stress in infertility has also been proposed by numerous authors (Agarwal 2005, Ruder 2009, Visioli 2011) and forms the focus of this present analysis.
Free radicals and oxidative stress
Free radicals, comprising two main classes of reactive oxygen species (ROS) and reactive nitrogen species (RNS) are unstable compounds that are produced through many physiological processes. While they are essential to some functions of the body such as infection control (Valko 2007), free radicals have the potential to cause significant tissue damage and disease. For this reason, mechanisms within the body work to stabilize free radicals and to neutralize the damage they may cause. Antioxidant compounds and enzymes accomplish this function on an ongoing basis (Agarwal 2005). When the burden of reactive species overwhelms the compensatory mechanisms of the body, oxidative stress occurs, causing damage to cellular structures and DNA (Valko 2007).
Oxidative processes in reproduction
As in the rest of the body, oxidative processes are integral to the proper functioning of the reproductive system. Key functions such as follicle and oocyte follicular development, embryonic development and implantation (Agarwal 2005, Wiener-Megnazi 2011) involve ROS. However, as oxidative stress has also been implicated as a causative factor in age-related fertility decline (Keefe 2009), it is clear that oxidative processes are not wholly supportive of reproductive processes.
Oxidative stress and endometriosis
Oxidative stress has been put forth as a contributing factor in women with endometriosis, a significant cause of female infertility (Augoulea 2009). Women with this presentation have been found to have a lower antioxidant capacity, as evidenced by decreased levels of plasma superoxide dismustase in one recent investigation (Prieto 2012). Oxidative processes, originating in the peritoneum, are thought to contribute to the development of endometriosis (Gupta 2005, Lousse 2012) and affect not only the structure of the reproductive tract, but oocyte quality in these women (Saito 2002). It has also been suggested that more advanced cases are associated with more evidence of systemic oxidative stress (Andrade 2010).
The administration of antioxidant therapies may provide a novel strategy for the management of this reproductive concern. One recent trial demonstrated that levels of malondialdehyde (MDA), a marker of oxidative stress, could be significantly attenuated by low doses of vitamins A and E (343mg and 84mg respectively) over a six-month period (Mier-Cabrera 2008). At the end of the study, pregnancy rates were slightly higher in the treatment group but results did not reach significance. Future trials with higher doses of targeted antioxidant compounds may hold promise in the treatment of this common cause of female infertility.
Recurrent pregnancy loss (RPL)
Recurrent pregnancy loss, the spontaneous termination of three or more pregnancies under 20 weeks gestation (Gupta 2007), may also prove to have an association with oxidative mechanisms. One study of 45 women that had experienced recurrent pregnancy loss found significantly decreased total antioxidant capacity (TAC) and increased total oxidative status (TOS) among these women compared to healthy pregnant controls (Toy 2010). This evidence is supported by an earlier study identifying low activity of the paraoxonase-1 enzymatic system that prevents lipid oxidation compared to healthy controls (p<0.01). High levels of lipid hydroperoxide in these same women demonstrated increased levels of oxidative stress in these individuals (p<0.01). It should be noted here that other studies have identified oxidative stress as a result rather than a cause of RPL (Baban 2010).
N-acetyl cysteine (NAC) is a mucolytic compound that has been discussed previously in reference to its application in polycystic ovarian syndrome (PCOS) (Flower 2011), where it appears to improve insulin sensitivity and reduce resistance to clomiphene therapy (Abu Hashim 2010). A recent prospective study (Amin 2008) assessed the suitability of NAC in the treatment of RPL, reporting a significant decrease in the risk of pregnancy loss when treatment with a combination of NAC (0.6g) and folic acid (500mcg) was initiated at the time of pregnancy confirmation. In comparison to folic acid therapy alone, the addition of NAC greatly improved the rate of pregnancy maintenance up to 20 weeks (RR 2.9, 95% confidence interval (CI) 1.5-5.6). Perhaps most importantly, the so-called take home baby rate was significantly higher in the NAC-treated group (RR 1.98, 95%CI 1.3-4.0).
Given the established antioxidant activity of NAC (Amin 2008), coupled with the evidence of increased oxidative stress in women suffering RPL, it is reasonable to postulate that this intervention improved pregnancy outcomes by attenuating the predominance of oxidative reactions in the body. It is not yet known whether this effect is achieved through direct action of NAC as a scavenger of free radicals or whether it counters oxidation more indirectly by increasing endogenous glutathione levels (Amin 2008). NAC and other antioxidants may have an important role to play in the management of this devastating condition.
Oxidative factors and in-vitro fertilization (IVF)
IVF, with or without intracytoplasmic sperm injection (ICSI), provides hope for many couples struggling with fertility challenges. A review of the literature pertaining to the oxidative status of women undergoing IVF indicates that this population may be another arena where intervention with antioxidant therapies may be appropriate.
Observational data from a series of prospective trials have examined markers of oxidative activity in women undergoing both IVF and ICSI (Bedaiwy 2010, Bedaiwy 2011, Liu 2010) and their relationship to pregnant cycles. All reviewed trials report similar findings. In their assessment of follicular fluid, Bedaiwy et al. (2011) report significant associations between both lower levels of ROS and higher TAC and pregnant cycles. Non-pregnant patients in the study by Liu et al. had higher MDA measurements (p<0.05) and lower SOD levels (p<0.05), indicating higher amounts of oxidative activity. An earlier study of ROS levels in embryo culture dishes found that lower levels on day three were significantly associated with pregnant cycles (Bedaiwy 2010). A milieu dominated by oxidative processes does not appear to favour conception.
Some researchers have taken this concept of hindrance by oxidation a step further and have declared a cut point for ROS levels in follicular fluid (Jana 2010). After assessing ROS in women with a range of fertility concerns (PCOS, endometriosis, tubal factor infertility), Jana et al. propose that ROS levels over 107cps/400micromol follicular fluid do not favour the growth of viable embryos. One may speculate that these findings could eventually translate into improved clinical tools for predicting IVF success rates.
Melatonin and IVF
Melatonin is a hormone that is naturally secreted by the pineal gland to manage sleep/wake cycles in humans. This compound has also been studied extensively for its antioxidant properties (Tan 2007). In light of the evidence suggesting a detrimental effect of oxidation in IVF cycles, it is not surprising that this antioxidant hormone may promote favourable outcomes for individuals undergoing this therapy.
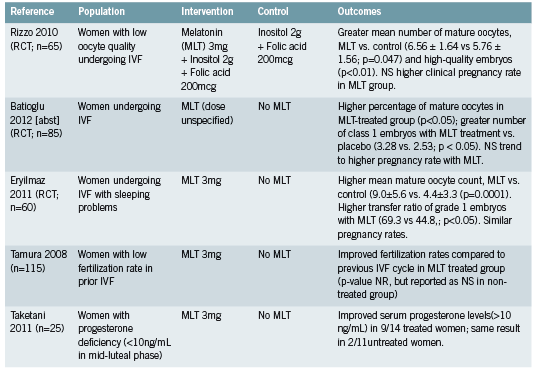
Three recent randomized controlled trials (RCTs) have evaluated the effect of 3mg of melatonin upon IVF-related parameters (Eryilmaz 2011, Rizzo 2010, Tamura 2008). A fourth trial did not specify dose in the abstract that was available for review (Batioğlu 2012). Trials reported significantly higher numbers of mature oocytes at pickup and higher quality embryos in treated patients (Batioğlu 2012, Rizzo 2010, Eryilmaz 2011). Trends towards higher pregnancy rates were also reported. When comparing current and previous IVF cycles, improved fertilization rates were seen among participants receiving melatonin (Tamura 2008).
The benefit of melatonin to parameters of successful IVF therapy may be attributed at least in part to its action as an antioxidant (Eryilmaz 2011, Rizzo 2010). This theory is supported and elaborated upon by a randomized trial (Taketani 2011) that demonstrates a protective effect of melatonin against reactive oxygen species (ROS) such as H2O2. The production of progesterone by luteinized granulosa cells was inhibited in vitro by H2O2 but this effect was reversed with the addition of melatonin. This effect was demonstrated in vivo by the same authors, through the restoration of deficient progesterone levels in some participants treated with 3mg of melatonin (see Figure 1).
Viewed from this perspective, melatonin may benefit women undergoing IVF, and presumably those trying to conceive naturally as well, through two related mechanisms. First, acting as a free-radical scavenger, melatonin may quench some of the oxidative stress that has been shown to be higher in women with diverse fertility challenges. Secondly, melatonin may reduce the activity of ROS such as H2O2 at the level of the ovary, preventing interference with endogenous progesterone production.
Future directions – CoQ10
While intervention studies have not yet been conducted, coenzyme Q10 (CoQ10) is another antioxidant that may also hold some promise in the treatment of infertility. A recent study investigated CoQ10 levels in the follicular fluid of women undergoing oocyte retrieval. Women with higher levels of CoQ10 had significantly increased numbers of mature oocytes and grade I-II embryos (Turi 2012), suggesting that the presence of this antioxidant compound may also contribute to positive fertility-associated outcomes.
Conclusions
Although oxidative processes are required for numerous essential physiological functions, a state of oxidative stress appears to be associated with conditions that may present barriers to successful conception. Markers of oxidative activity may be higher in women with endometriosis and a history of EPL. While antioxidant therapy has not been fully evaluated for either condition, treatment with 600mg of NAC may help women with EPL to prolong and preserve their pregnancies.
In women undergoing IVF treatments, increased levels of oxidative stress have been observed and may be associated with the success of individual IVF cycles. Melatonin administration at a dose of 3mg per night has been significantly associated with improved oocyte maturity and embryo quality. CoQ10 may also contribute positively to these outcomes but intervention studies are needed to support observational data. While the association between oxidation and female fertility is not entirely understood, this relationship offers some novel therapeutic options to care providers and may further our understanding of infertility that is otherwise unexplained.
References
Abu Hashim H, Anwar K, El-Fatah RA. N-acetyl cysteine plus clomiphene citrate versus metformin and clomiphene citrate in treatment of clomiphene-resistant polycystic ovary syndrome: a randomized controlled trial. J Womens Health (Larchmt). 2010 Nov;19(11):2043-8.
Agarwal A, Gupta S, Sharma RK. Role of oxidative stress in female reproduction.ReprodBiolEndocrinol. 2005 Jul 14;3:28.
Amin AF, Shaaban OM, Bediawy MA. N-acetyl cysteine for treatment of recurrent unexplained pregnancy loss.Reprod Biomed Online. 2008 Nov;17(5):722-6.
Andrade AZ, Rodrigues JK, Dib LA, Romão GS, Ferriani RA, Jordão Junior AA, Navarro PA.[Serum markers of oxidative stress in infertile women with endometriosis]. [Article in Portuguese] Rev Bras Ginecol Obstet. 2010 Jun;32(6):279-85.
Assisted Human Reproduction Canada (AHRC). Infertility and Assisted Human Reproduction (AHR) [Internet] 2010 Aug 26 [cited 2012 Sep 23]. Available from: http://www.ahrc-pac.gc.ca/v2/patients/infertilityinfertilite- eng.php
Augoulea A, Mastorakos G, Lambrinoudaki I, Christodoulakos G, Creatsas G. The role of the oxidative-stress in the endometriosis-related infertility.GynecolEndocrinol. 2009 Feb;25(2):75-81.
Baban RS. Oxidative stress in recurrent pregnancy loss women. Saudi Med J. 2010 Jul;31(7):759-63.
Batioğlu AS, Sahin U, Gürlek B, Oztürk N, Unsal E. The efficacy of melatonin administration on oocyte quality.GynecolEndocrinol. 2012 Feb;28(2):91-3. [abst]
Bedaiwy MA, Elnashar SA, Goldberg JM, Sharma R, Mascha EJ, Arrigain S, Agarwal A, Falcone T. Effect of follicular fluid oxidative stress parameters on intracytoplasmic sperm injection outcome. GynecolEndocrinol. 2012 Jan;28(1):51-5.
Bedaiwy MA, Mahfouz RZ, Goldberg JM, Sharma R, Falcone T, Abdel Hafez MF, Agarwal A. Relationship of reactive oxygen species levels in day 3 culture media to the outcome of in vitro fertilization/intracytoplasmic sperm injection cycles.FertilSteril. 2010 Nov;94(6):2037-42.
Bushnik T, Cook JL, Yuzpe AA, Tough S, Collins J. Estimating the prevalence of infertility in Canada. Hum Reprod. 2012 Mar;27(3):738- 46.
Eloualid A, Abidi O, Charif M, El Houate B, Benrahma H, Louanjli N, Chadli E, Ajjemami M, Barakat A, Bashamboo A, McElreavey K, Rhaissi H, Rouba H. Association of the MTHFR A1298C variant with unexplained severe male infertility. PLoS One. 2012;7(3):e34111.
Eryilmaz OG, Devran A, Sarikaya E, Aksakal FN, Mollamahmutoğlu L, Cicek N. Melatonin improves the oocyte and the embryo in IVF patients with sleep disturbances, but does not improve the sleeping problems. J Assist Reprod Genet. 2011 Sep;28(9):815-20.
Flower G. Polycystic ovarian syndrome – Clinical considerations and therapeutic options. Integrated Healthcare Practitioners. 2011 April/ May;20:68-72.
Gupta S, Agarwal A, Banerjee J, Alvarez JG. The role of oxidative stress in spontaneous abortion and recurrent pregnancy loss: a systematic review. ObstetGynecolSurv. 2007 May;62(5):335-47; quiz 353-4.
Gupta S, Agarwal A, Krajcir N, Alvarez JG. Role of oxidative stress in endometriosis.Reprod Biomed Online. 2006 Jul;13(1):126-34.
Jana SK, K NB, Chattopadhyay R, Chakravarty B, Chaudhury K. Upper control limit of reactive oxygen species in follicular fluid beyond which viable embryo formation is not favorable. ReprodToxicol. 2010 Jul;29(4):447-51.
Keefe DL, Liu L. Telomeres and reproductive aging.ReprodFertil Dev. 2009;21(1):10-4. Ledger WL. Demographics of infertility.Reprod Biomed Online. 2009;18Suppl 2:11-4.
Liu J, Li Y. [Effect of oxidative stress and apoptosis in granulosa cells on the outcome of IVF-ET]. [Article in Chinese] Zhong Nan Da XueXueBao Yi Xue Ban. 2010 Sep;35(9):990-4. [abst]
Lousse JC, Van Langendonckt A, Defrere S, Ramos RG, Colette S, Donnez J. Peritoneal endometriosis is an inflammatory disease. Front Biosci (Elite Ed). 2012 Jan 1;4:23-40.
Mier-Cabrera J, Genera-García M, De la Jara-Díaz J, Perichart- Perera O, Vadillo-Ortega F, Hernández-Guerrero C. Effect of vitamins C and E supplementation on peripheral oxidative stress markers and pregnancy rate in women with endometriosis. Int J Gynaecol Obstet. 2008 Mar;100(3):252-6.
Practice Committee of the American Society for Reproductive Medicine (PCASRM). Definitions of infertility and recurrent pregnancy loss. FertilSteril. 2008 Nov;90(5 Suppl):S60.
Prieto L, Quesada JF, Cambero O, Pacheco A, Pellicer A, Codoceo R, Garcia-Velasco JA. Analysis of follicular fluid and serum markers of oxidative stress in women with infertility related to endometriosis. FertilSteril. 2012 Jul;98(1):126-30.
Rizzo P, Raffone E, Benedetto V. Effect of the treatment with myoinositol plus folic acid plus melatonin in comparison with a treatment with myo-inositol plus folic acid on oocyte quality and pregnancy outcome in IVF cycles. A prospective, clinical trial.Eur Rev Med Pharmacol Sci. 2010 Jun;14(6):555-61.
Ruder EH, Hartman TJ, Goldman MB.Impact of oxidative stress on female fertility.CurrOpinObstet Gynecol. 2009 Jun;21(3):219-22.
Sadeu JC, DoedéeAM, Neal MS, Hughes EG, Foster WG. Neurotrophins (BDNF and NGF) in follicular fluid of women with different infertility diagnoses.Reprod Biomed Online. 2012 Feb;24(2):174-9.
Saito H, Seino T, Kaneko T, Nakahara K, Toya M, Kurachi H. Endometriosis and oocyte quality. GynecolObstet Invest. 2002;53Suppl 1:46-51.
Siam EM, Hefzy EM.The relationship between antisperm antibodies prevalence and genital chlamydia trachomatis infection in women with unexplained infertility.Afr J Reprod Health. 2011 Sep;15(3):93-101.
Taketani T, Tamura H, Takasaki A, Lee L, Kizuka F, Tamura I, Taniguchi K, Maekawa R, Asada H, Shimamura K, Reiter RJ, Sugino N. Protective role of melatonin in progesterone production by human luteal cells. J Pineal Res. 2011 Sep;51(2):207-13. doi: 10.1111/j.1600- 079X.2011.00878.x. [abst]
Tamura H, Takasaki A, Miwa I, Taniguchi K, Maekawa R, Asada H, Taketani T, Matsuoka A, Yamagata Y, Shimamura K, Morioka H, Ishikawa H, Reiter RJ, Sugino N. Oxidative stress impairs oocyte quality and melatonin protects oocytes from free radical damage and improves fertilization rate. J Pineal Res. 2008 Apr;44(3):280-7. [abst]
Tan DX, Manchester LC, Terron MP, Flores LJ, Reiter RJ. One molecule, many derivatives: a never-ending interaction of melatonin with reactive oxygen and nitrogen species? J Pineal Res. 2007 Jan;42(1):28-42.
Toy H, Camuzcuoglu H, Camuzcuoglu A, Celik H, Aksoy N. Decreased serum prolidase activity and increased oxidative stress in early pregnancy loss. GynecolObstet Invest. 2010;69(2):122-7.
Turi A, Giannubilo SR, Brugè F, Principi F, Battistoni S, Santoni F, Tranquilli AL, Littarru G, Tiano L.Coenzyme Q10 content in follicular fluid and its relationship with oocyte fertilization and embryo grading. Arch Gynecol Obstet. 2012 Apr;285(4):1173-6.
Valko M, Leibfritz D, Moncol J, Cronin MT, Mazur M, Telser J. Free radicals and antioxidants in normal physiological functions and human disease. Int J Biochem Cell Biol. 2007;39(1):44-84.
Visioli F, Hagen TM. Antioxidants to enhance fertility: role of eNOS and potential benefits. Pharmacol Res. 2011 Nov;64(5):431-7.
Wiener-Megnazi Z, Reznick AZ, Lahav-Baratz S, Shiloh H, Koifman M, Grach B, Arnon T, Avraham L, Auslander R, Dirnfeld M. [Oxidation and female reproduction: the good, the bad and what’s between]. [Article in Hebrew] Harefuah. 2011 Mar;150(3):255-9, 303.





