
L- Carnitine
Heidi Fritz MA, ND
Introduction
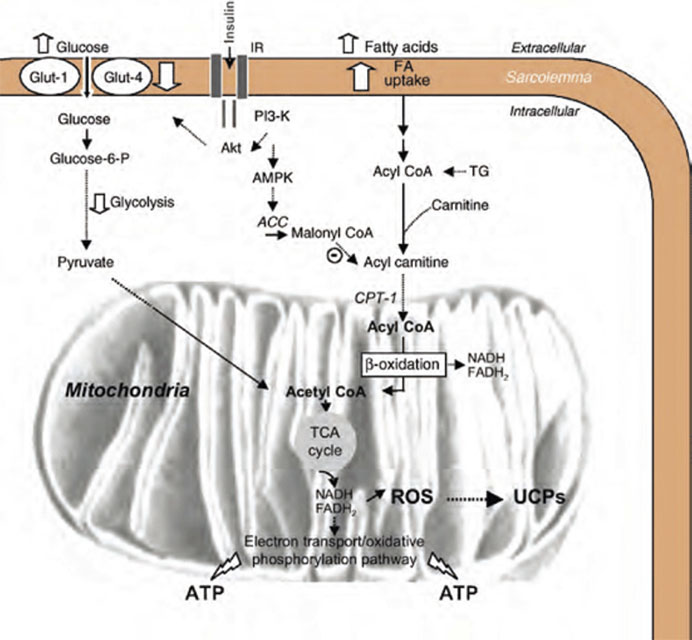
L-carnitine is a trimethylated amino acid- derivative whose most well described biological function is as a cofactor of fatty acid metabolism (Alt Med Rev 2005). L-carnitine is a key component of the intracellular shuttle system that transports free fatty acids from the cytosol and across the mitochondrial membrane where they undergo beta oxidation and transformation to ATP (Karlic 2004). Long chain fatty acids represent up to 80% of the body’s energy sources during most physiological states with the exception of high intensity exercise (Karlic 2004) and are the preferred substrate in cardiac muscle (Carvajal 2003). L-carnitine also impacts other cellular energy- producing pathways (Mate 2010). Optimization of mitochondrial metabolism through supplementation with L-carnitine, which is known to concentrate in cardiac and skeletal muscle (Flanagan 2010), could be an effective intervention for a variety of conditions characterized by fatigue, pain, and impaired muscle function. This paper focuses on the evidence base for L-carnitine in cardiovascular medicine.
Physiology
L-carnitine is considered to be conditionally essential, meaning that although there are rare genetic conditions causing primary deficiency, and secondary deficiency resulting commonly from hemodialysis in patients with kidney disease, most healthy individuals can synthesize L-carnitine from dietary lysine and methionine and cofactors vitamin C, iron, pyroxidine, and niacin (Flanagan 2010, Mate 2010). Despite this, alterations of L-carnitine metabolism are common in cardiovascular disease, most likely due to a combination of increased utilization and the inability of myocardiocytes to synthesize carnitine endogenously.
Cardiac ischemia is well recognized in the literature to be accompanied by a rapid depletion in myocardial carnitine content and a concurrent rise in intracellular long chain free fatty acids (Gurlek 2000, Regitz 1990A, Regitz 1990B, Tarantini 2006). In patients with heart failure, serum carnitine has been correlated with impaired left ventricular systolic function as measured by echocardiography (El-Aroussy 2000). During ischemia L-carnitine is thought to offset rising concentrations of free fatty acids by facilitating mitochondrial uptake and utilization, thereby preventing the damaging effects of elevated free fatty acids: membrane damage with consequent cell swelling and microvascular compression, arrhythmias, and metabolic inefficiency with consequent deterioration of myocardial function (Tarantini 2006).
In addition to its facilitating fatty acid transport into the mitochondria, L-carnitine performs a second key metabolic function: the removal from the mitochondria of short and medium chain fatty acids (acetyl groups) formed as products of beta oxidation and bound to CoA as acetyl-CoA (Mate 2010). Mitochondrial accumulation of this byproduct is toxic, inhibiting pyruvate dehydrogenase activity and glucose oxidation. On the other hand, the removal of acetyl groups and consequent increase in free CoA stimulates energy production through the Kreb’s cycle (Mate 2010). In this way, L-carnitine can regulate both fatty acid and glucose metabolism in ischemic cardiac tissue. See Figure 1. Importantly, since myocardium is unable to synthesize carnitine itself, exogenous administration may be necessary to restore optimal levels and metabolic function.
Human Evidence
Oral and intravenous L-carnitine has been shown to be benefi cial for a number of cardiovascular conditions including angina (Bartels 1996, Cacciatore 1991), acute myocardial infarction (Gurlek 2000), chronic heart failure (Rizos 2000), and peripheral vascular disease (Brevetti 1999); because it is more accessible, this summary focuses on oral L-carnitine in particular. e typical dosage is 2g per day in divided doses (Gurlek 2000, Singh 1996); some studies have used up to 6g per day (Iliceto 1995). No adverse events beyond mild gastrointestinal upset, which was rare, were reported (Kumar 2007). It should be noted that most of the studies cited here included patients also receiving standard medications for their conditions, and that L-carnitine was studied as an “add on” therapy; space constraints limit the detail in which this can be described for each study.
Angina ere are at least eight controlled human trials of oral L-carnitine for the treatment of angina. Of these, all found benefi t (Bartels 1995, Bartels 1996, Cacciatore 1991, Cherchi 1985, Cherchi 1990, Iyer 2000, Kamikawa 1984, Lagioia 1992, McMackin 2007). L carnitine has been shown to:
• Improve cardiac function (eg. cardiac output, maximal heart rate) during exercise and improve overall exercise performance (eg. exercise time, exercise workload) despite having no eff ect on myocardial oxygen requirements (Bartels 1996, Bartels 1995, Cacciatore 1991, Cherchi 1985, Iyer 2000, Kamikawa 1984, Lagioia 1992);
• Reduce myocardial ischemia upon exercise testing, measured as the time to ST-segment depression or the degree of ST-depression on ECG (Bartels 1996, Bartels 1995, Cacciatore 1991, Cherchi 1985, Cherchi 1990, Kamikawa 1984, Lagioia 1992);
• Reverse angina, with a number of patients becoming angina- free during treatment (up to 22.7% of patients compared to 9.1% in the placebo group according to Cherchi 1985, 2 out of 12 patients according to Kamikawa 1984); • Decrease frequency of angina attacks by up to 70% and nitroglycerin consumption by 57% according to Bartels 1996, comparable to treatment with diltiazem;
• One additional study in patients without angina but with established coronary artery disease showed L-carnitine to increase brachial artery diameter by 2.3%, consistent with reduced arterial tone (McMackin 2007).
L-carnitine exerts these eff ects without reducing myocardial oxygen demand, as do select cardiac medications such as beta blockers. Bartels showed that: “[proprionyl-L-carnitine] prevents ischemia-induced ventricular dysfunction, not by aff ecting the myocardial oxygen supply-demand ratio but as a result of its intrinsic metabolic actions, increasing pyruvate dehydrogenase activity and fl ux through the citric acid cycle” (1994).
Acute Myocardial Infarction
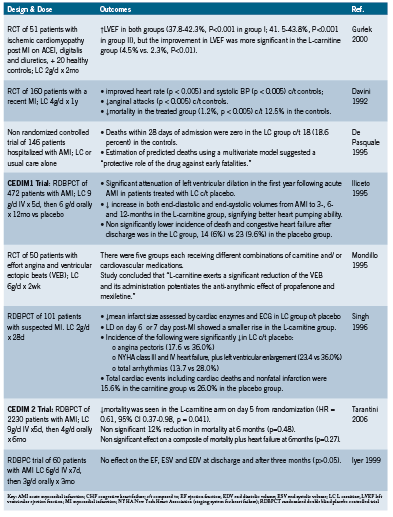
Eight controlled trials have examined the eff ect of L-carnitine in the treatment of acute myocardial infarction (AMI), often with intravenous administration for an initial period, followed by long term oral administration. ese are summarized in Table 1. When added to standard therapies, L-carnitine has been found to:
• Improve myocardial pumping ability: increasing left ventricular ejection fraction (LVEF) (Gurlek 2000), and end- diastolic and end- systolic volumes (Iliceto 1995)
• Reduce myocardial damage: reduced infarct size when administered acutely (Singh 1996), and reduced deleterious left ventricular remodeling and dilation when administered acutely and long term (Iliceto 1995)
• Decrease angina following MI by up to half that experienced by patients receiving placebo (Davini 1992, Singh 1996)
• Decrease incidence of arrhythmias following MI (Mondillo 1995, Singh 1996)
• Reduce number of second cardiac events to 15.6%, compared to 26% in placebo (Singh 1996)
• Reduce overall mortality, with 1.2% rate reported in LC group compared to 12.5% in the placebo group according to Davini 1992. Reduced mortality also demonstrated by De Pasquale (1995).
Two large randomized controlled trials have been conducted by Italian researchers. The CEDIM1 (Carnitine Ecocardiografia Digitalizzata Infarto Miocardico) and CEDIM2 trials investigated the use of intravenous L-carnitine 9g/d for the first five days after AMI, followed by 4 to 6 g/d orally for 6 to 12 months in 472 and 2230 patients respectively (Iliceto 1995, Tarantini 2006). Although the studies differed in their long term (6-12 months) findings, both demonstrate that L-carnitine can reduce early mortality post AMI. CEDIM2 found significantly reduced early mortality, risk of death at 5 days HR 0.61 (95% CI 0.37-0.98), and upon reanalysis, it was found that much of the apparent benefit seen in CEDIM1 was also due to lower early mortality (Tarantini 2006).
Of the eight studies, seven found significant positive effects (Davini 1992, De Pasquale 1995, Gurlek 2000, Iliceto 1995, Mondillo 1995, Singh 1996, Tarantini 2006). Iyer found no effect on cardiac function in a smaller trial of 60 patients using L-carnitine 6g/d intravenously for the first 7 days, then 3g/d orally for 3 months, and it has been suggested that this may be due to the smaller trial size compared to CEDIM 1 and 2, or the lower dosage used (1999).
Heart Failure
Nine controlled trials have investigated L-carnitine for patients with chronic/ congestive heart failure (CHF) (Anand 1998, Caponetto 1994, Ghidini 1988, Kumar 2007, Loster 1999, Mancini 1992, No authors 1999, Pucciarelli 1992, Rizos 2000). L-carnitine has been shown to:
• Improve exercise performance (maximum exercise time) (Caponetto 1994, Kumar 2007, Loster 1999, Mancini 1992, No authors 1999, Pucciarelli 1992, Rizos 2000)
• Improve cardiac function during exercise (eg. peak exercise heart rate, ejection fraction) (Anand 1998, Mancini 1992, No authors 1999)
• Increase cardiac pumping ability (eg. cardiac output, stroke volume index, left ventricular ejection fraction, pulmonary blood pressure) (Caponetto 1994, Pucciarelli 1992, Rizos 2000)
• Decrease left ventricular size (Anand 1998)
• Decrease signs and symptoms associated with CHF, including dyspnea, palpitations, fatigue, edema, and improved diuresis (Ghidini 1988, Kumar 2007)
• Reduce long term mortality: in one study 3-year mortality was 3% for patients receiving L-carnitine, compared to 18% for those on placebo (p<0.04) (Rizos 2000).
Interestingly, Loster found that the beneficial effects of L-carnitine continued to persist for up to 60 days after cessation of treatment (1999).
Peripheral Vascular Disease Nine controlled trials have investigated L-carnitine, mostly as proprionyl-L-carnitine (PLC), for the treatment of peripheral vascular diseases secondary to smoking or diabetes (Barker 2001, Brevetti 1999, Brevetti 1997, Brevetti 1995, Brevetti 1988, Dal Lago 1999, Greco 1992, Hiatt 2001, Santo 2006). PLC appears to benefit predominantly those patients with moderate to severe disease, with limited effect in mild disease (Brevetti 1999, 1997, Silvestro 2006). PLC has been shown to:
• Increase walking time and/ or distance, by up to 98% in those with moderate to severe disease (Brevetti 1999, Brevetti 1995, Brevetti 1988, Dal Lago 1999, Greco 1992, Hiatt 2001)
• Increase intermittent claudication distance (the distance walked until onset of claudication) (Brevetti 1999, Santo 2006)
• Improve ankle-brachial index (Greco 1992, Santo 2006)
• Improve quality of life (Brevetti 1997)
Intravenous PLC infused 3 times weekly has also been shown to augment the effects of a physical training program in patients with moderate to severe intermittent claudication (Andreozzi 2008). Biopsy of ischemic muscle has shown that supplementation with PLC increases muscle total carnitine content after 15 days (Brevetti 1988); and uncontrolled trials have shown an ability of PLC to attenuate cold induced decreases in blood flow in patients with vasospastic disease such as Raynaud’s (Gasser 1997) and reduce exercise induced increases in serum adhesion molecules, suggesting vasoprotective effects (Signorelli 2001).
Conclusion
L-carnitine is a necessary cofactor for mitochondrial function, stimulating oxidative metabolism of glucose and fatty acids particularly under conditions of ischemia. L-carnitine protects against ischemiainduced myocardial dysfunction and has been demonstrated to improve cardiac function and exercise performance in patients with angina, myocardial infarction, and heart failure. L-carnitine can decrease frequency of angina attacks; reduce deleterious cardiac remodeling and arrhythmias, and improve survival after MI; and decrease symptoms of CHF while increasing long term survival. L-carnitine also benefits peripheral vascular disease. L-carnitine has been administered alongside standard cardioactive medications in many of the trials described above without report of any serious adverse events, and can be safely considered for comanagement of the cardiac patient.
References
Acetyl-L-carnitine. Monograph. Altern Med Rev. 2010 Apr;15(1):76-83.
Anand I, Chandrashekhan Y, De Giuli F, Pasini E, Mazzoletti A, Confortini R, Ferrari R. Acute and chronic eff ects of propionyl-L-carnitine on the hemodynamics, exercise capacity, and hormones in patients with congestive heart failure. Cardiovasc Drugs er. 1998 Jul;12(3):291-9.
Andreozzi GM, Leone A, Laudani R, Martin R, Deinit G, Cataldi V. Levo-propionylcarnitine improves the eff ectiveness of supervised physical training on the absolute claudication distance in patients with intermittent claudication. Angiology. 2008 Feb-Mar;59(1):84-9.
Barker GA, Green S, Askew CD, Green AA, Walker PJ. Eff ect of propionyl-L-carnitine on exercise performance in peripheral arterial disease. Med Sci Sports Exerc. 2001 Sep;33(9):1415-22.
Bartels GL, Remme WJ, Holwerda KJ, Kruijssen DA. Anti-ischaemic effi cacy of Lpropionylcarnitine– a promising novel metabolic approach to ischaemia? Eur Heart J. 1996 Mar;17(3):414-20.
Bartels GL, Remme WJ, den Hartog FR, Wielenga RP, Kruijssen DA. Additional antiischemic eff ects of long-term L-propionylcarnitine in anginal patients treated with conventional antianginal therapy. Cardiovasc Drugs er. 1995 Dec;9(6):749-53.
Bartels GL, Remme WJ, Pillay M, Schönfeld DH, Kruijssen DA. Eff ects of L-propionylcarnitine on ischemia-induced myocardial dysfunction in men with angina pectoris. Am J Cardiol. 1994 Jul 15;74(2):125-30.
Brevetti G, Attisano T, Perna S, Rossini A, Policicchio A, Corsi M. Eff ect of L-carnitine on the reactive hyperemia in patients aff ected by peripheral vascular disease: a double-blind, crossover study. Angiology. 1989 Oct;40(10):857-62.
Brevetti G, Chiariello M, Ferulano G, Policicchio A, Nevola E, Rossini A, Attisano T, Ambrosio G, Siliprandi N, Angelini C. Increases in walking distance in patients with peripheral vascular disease treated with L-carnitine: a double-blind, cross-over study. Circulation. 1988 Apr;77(4):767-73.
Brevetti G, Diehm C, Lambert D. European multicenter study on propionyl-L-carnitine in intermittent claudication. J Am Coll Cardiol. 1999 Nov 1;34(5):1618-24.
Brevetti G, Perna S, Sabba C, Martone VD, Di Iorio A, Barletta G. Eff ect of propionyl-L-carnitine on quality of life in intermittent claudication. Am J Cardiol. 1997 Mar 15;79(6):777-80.
Brevetti G, Perna S, Sabba C, Martone VD, Condorelli M. Propionyl-L-carnitine in intermittent claudication: double-blind, placebo-controlled, dose titration, multicenter study. J Am Coll Cardiol. 1995 Nov 15;26(6):1411-6.
Cacciatore L, Cerio R, Ciarimboli M, Cocozza M, Coto V, D’Alessandro A, D’Alessandro L, Grattarola G, Imparato L, Lingetti M, et al. e therapeutic eff ect of L-carnitine in patients with exercise-induced stable angina: a controlled study. Drugs Exp Clin Res. 1991;17(4):225-35. [Abstr]
Caponnetto S, Canale C, Masperone MA, Terracchini V, Valentini G, Brunelli C. Effi cacy of L-propionylcarnitine treatment in patients with left ventricular dysfunction. Eur Heart J. 1994 Sep;15(9):1267-73.
Carvajal K, Moreno-Sánchez R. Heart metabolic disturbances in cardiovascular diseases. Arch Med Res. 2003 Mar-Apr;34(2):89-99.
Cherchi A, Lai C, Angelino F, Trucco G, Caponnetto S, Mereto PE, Rosolen G, Manzoli U, Schiavoni G, Reale A, et al. Eff ects of L-carnitine on exercise tolerance in chronic stable angina: a multicenter, double-blind, randomized, placebo controlled crossover study. Int J Clin Pharmacol er Toxicol. 1985 Oct;23(10):569-72. [Abstr]
Cherchi A, Lai C, Onnis E, Orani E, Pirisi R, Pisano MR, Soro A, Corsi M. Propionyl carnitine in stable eff ort angina. Cardiovasc Drugs er. 1990 Apr;4(2):481-6.
Dal Lago A, De Martini D, Flore R, Gaetani E, Gasbarrini A, Gerardino L, Pola R, Santoliquido A, Serricchio M, Tondi P, Nolfe G. Eff ects of propionyl-L-carnitine on peripheral arterial obliterative disease of the lower limbs: a double-blind clinical trial. Drugs Exp Clin Res. 1999;25(1):29-36.
Davini P, Bigalli A, Lamanna F, Boem A. Controlled study on L-carnitine therapeutic effi cacy in post-infarction. Drugs Exp Clin Res. 1992;18(8):355-65.
De Pasquale B, Righetti G, Menotti A. [L-carnitine for the treatment of acute myocardial infarct]. Cardiologia. 1990 Jul;35(7):591-6.
El-Aroussy W, Rizk A, Mayhoub G, Aleem SA, El-Tobgy S, Mokhtar MS. Plasma carnitine levels as a marker of impaired left ventricular functions. Mol Cell Biochem. 2000 Oct;213(1-2):37-41.
Flanagan JL, Simmons PA, Vehige J, Willcox MD, Garrett Q. Role of carnitine in disease. Nutr Metab (Lond). 2010 Apr 16;7:30.
Gasser P, Martina B, Dubler B. Reaction of capillary blood cell velocity in nailfold capillaries to L-carnitine in patients with vasospastic disease. Drugs Exp Clin Res. 1997;23(1):39-43.
Ghidini O, Azzurro M, Vita G, Sartori G. Evaluation of the therapeutic effi cacy of L-carnitine in congestive heart failure. Int J Clin Pharmacol er Toxicol. 1988 Apr;26(4):217-20. Erratum in: Int J Clin Pharmacol er Toxicol 1989 Aug;27(8):418.
Greco AV, Mingrone G, Bianchi M, Ghirlanda G. Eff ect of propionyl-L-carnitine in the treatment of diabetic angiopathy: controlled double blind trial versus placebo. Drugs Exp Clin Res. 1992;18(2):69-80.
Gürlek A, Tutar E, Akçil E, Dinçer I, Erol C, Kocatürk PA, Oral D. e eff ects of L-carnitine treatment on left ventricular function and erythrocyte superoxide dismutase activity in patients with ischemic cardiomyopathy. Eur J Heart Fail. 2000 Jun;2(2):189-93.
Hiatt WR, Regensteiner JG, Creager MA, Hirsch AT, Cooke JP, Olin JW, Gorbunov GN, Isner J, Lukjanov YV, Tsitsiashvili MS, Zabelskaya TF, Amato A. Propionyl-L-carnitine improves exercise performance and functional status in patients with claudication. Am J Med. 2001 Jun 1;110(8):616-22.
Iliceto S, Scrutinio D, Bruzzi P, D’Ambrosio G, Boni L, Di Biase M, Biasco G, Hugenholtz PG, Rizzon P. Eff ects of L-carnitine administration on left ventricular remodeling after acute anterior myocardial infarction: the L-Carnitine Ecocardiografi a Digitalizzata Infarto Miocardico (CEDIM) Trial. J Am Coll Cardiol. 1995 Aug;26(2):380-7.
Iyer RN, Khan AA, Gupta A, Vajifdar BU, Lokhandwala YY. L-carnitine moderately improves the exercise tolerance in chronic stable angina. J Assoc Physicians India. 2000 Nov;48(11):1050-2.
Iyer R, Gupta A, Khan A, Hiremath S, Lokhandwala Y. Does left ventricular function improve with L-carnitine after acute myocardial infarction? J Postgrad Med. 1999 Apr-Jun;45(2):38-41.
Karlic H, Lohninger A. Supplementation of L-carnitine in athletes: does it make sense? Nutrition. 2004 Jul-Aug;20(7-8):709-15.
Kamikawa T, Suzuki Y, Kobayashi A, Hayashi H, Masumura Y, Nishihara K, Abe M, Yamazaki N. Eff ects of L-carnitine on exercise tolerance in patients with stable angina pectoris. Jpn Heart J. 1984 Jul;25(4):587-97.
Kumar A, Singh RB, Saxena M, Niaz MA, Josh SR, Chattopadhyay P, Mechirova V, Pella D, Fedacko J. Eff ect of carni Q-gel (ubiquinol and carnitine) on cytokines in patients with heart failure in the Tishcon study. Acta Cardiol. 2007 Aug;62(4):349-54.
Lagioia R, Scrutinio D, Mangini SG, Ricci A, Mastropasqua F, Valentini G, Ramunni G, Totaro Fila G, Rizzon P. Propionyl-L-carnitine: a new compound in the metabolic approach to the treatment of eff ort angina. Int J Cardiol. 1992 Feb;34(2):167-72. [Abstr]
Löster H, Miehe K, Punzel M, Stiller O, Pankau H, Schauer J. Prolonged oral L-carnitine substitution increases bicycle ergometer performance in patients with severe, ischemically induced cardiac insuffi ciency. Cardiovasc Drugs er. 1999 Nov;13(6):537-46.
Mancini M, Rengo F, Lingetti M, Sorrentino GP, Nolfe G. Controlled study on the therapeutic effi cacy of propionyl-L-carnitine in patients with congestive heart failure. Arzneimittelforschung. 1992 Sep;42(9):1101-4.
Mate A, Miguel-Carrasco JL, Vázquez CM. e therapeutic prospects of using L-carnitine to manage hypertension-related organ damage. Drug Discov Today. 2010 Jun;15(11-12):484-92.
McMackin CJ, Widlansky ME, Hamburg NM, Huang AL, Weller S, Holbrook M, Gokce N, Hagen TM, Keaney JF Jr, Vita JA. Eff ect of combined treatment with alpha-Lipoic acid and acetyl-L-carnitine on vascular function and blood pressure in patients with coronary artery disease. J Clin Hypertens (Greenwich). 2007 Apr;9(4):249-55.
Mondillo S, Faglia S, D’Aprile N, Mangiacotti L, Campolo MA, Agricola E, Palazzuoli V. [ erapy of arrhythmia induced by myocardial ischemia. Association of L-carnitine, propafenone and mexiletine]. Clin Ter. 1995 Dec;146(12):769-74. [Abstr]
No authors. Study on propionyl-L-carnitine in chronic heart failure. Eur Heart J. 1999 Jan;20(1):70-6.
Pucciarelli G, Mastursi M, Latte S, Sacra C, Setaro A, Lizzadro A, Nolfe G. [ e clinical and hemodynamic eff ects of propionyl-L-carnitine in the treatment of congestive heart failure]. Clin Ter. 1992 Nov;141(11):379-84. [Abstr]
Regitz V, Bossaller C, Strasser R, Müller M, Shug AL, Fleck E. Metabolic alterations in endstage and less severe heart failure–myocardial carnitine decrease. J Clin Chem Clin Biochem. 1990 Sep;28(9):611-7. A
Regitz V, Shug AL, Fleck E. Defective myocardial carnitine metabolism in congestive heart failure secondary to dilated cardiomyopathy and to coronary, hypertensive and valvular heart diseases. Am J Cardiol. 1990 Mar 15;65(11):755-60. B
Rizos I. ree-year survival of patients with heart failure caused by dilated cardiomyopathy and L-carnitine administration. Am Heart J. 2000 Feb;139(2 Pt 3):S120-3.
Santo SS, Sergio N, Luigi DP, Giuseppe M, Margherita F, Gea OC, Roberto F, Gabriella C, Giuseppe P, Massimiliano A. Eff ect of PLC on functional parameters and oxidative profi le in type 2 diabetes-associated PAD. Diabetes Res Clin Pract. 2006 Jun;72(3):231-7.
Signorelli SS, Malaponte G, Di Pino L, Digrandi D, Pennisi G, Mazzarino MC. Eff ects of ischaemic stress on leukocyte activation processes in patients with chronic peripheral occlusive arterial disease: role of L-propionyl carnitine administration. Pharmacol Res. 2001 Oct;44(4):305-9.
Singh RB, Niaz MA, Agarwal P, Beegum R, Rastogi SS, Sachan DS. A randomised, doubleblind, placebo-controlled trial of L-carnitine in suspected acute myocardial infarction. Postgrad Med J. 1996 Jan;72(843):45-50.
Tarantini G, Scrutinio D, Bruzzi P, Boni L, Rizzon P, Iliceto S. Metabolic treatment with L-carnitine in acute anterior ST segment elevation myocardial infarction. A randomized controlled trial. Cardiology. 2006;106(4):215-23.








